
PATHOGENESIS AND CURRENT METHODS OF TREATMENT OF SECONDARY UVEITIC GLAUCOMA. A REVIEW
Authors:
E. Škrlová; P. Svozílková; J. Heissigerová; M. Fichtl
Authors‘ workplace:
Oční klinika, 1. lékařská fakulta, Univerzita Karlova a Všeobecná fakultní nemocnice v Praze
Published in:
Čes. a slov. Oftal., 79, 2023, No. 3, p. 111-115
Category:
Review Article
doi:
https://doi.org/10.31348/2023/7
Overview
Secondary uveitic glaucoma is a serious sight-threatening complication of intraocular inflammation (uveitis). It develops in approximately 10–20% of patients with uveitis (although this figure may be higher depending on the type of inflammation). It is more commonly associated with chronic forms of uveitis, especially anterior uveitis. Elevation of intraocular pressure (IOP) and the development of secondary glaucoma arise as a direct or indirect consequence of uveitis, and may develop further in association with therapy for intraocular inflammation. Several types of uveitic glaucoma are distinguished according to the mechanism of development: open-angle secondary glaucoma (including steroid-induced secondary glaucoma), angle-closure secondary glaucoma, and a combination of both. It is necessary to determine the pathogenesis of uveitis and target the treatment of the inflammatory process according to it. Subsequently, it is necessary to determine the type of secondary glaucoma, which influences the choice of therapy. Compensation for IOP should be achieved as quickly as possible, before irreversible damage to the optic nerve and visual field occurs. In the first instance, we choose conservative pharmacological therapy. However, this therapy fails more often in secondary uveitic glaucoma than in primary open-angle glaucoma. For this reason, surgical or laser therapy is necessary for refractory glaucoma. Trabeculectomy remains the gold standard in surgical therapy for secondary uveitic glaucoma, but other surgical techniques can also be used (Ahmed drainage implants, goniotomy in the paediatric population, surgical iridectomy, and synechiae for angle closure etc.). The choice of method is individualised according to the clinical findings of the patient and previous ocular procedures. However, the main factor influencing the success and efficacy of filtration surgery is adequate therapy and control of the intraocular inflammatory process.
Keywords:
Uveitis – secondary uveitic glaucoma – therapy of secondary uveitic glaucoma

INTRODUCTION
Secondary uveitic glaucoma is a serious and relatively common complication of intraocular inflammations (uveitis). It is defined as an increase of intraocular pressure (IOP) in patients with uveitis, which leads to damage to the optic nerve and causes a progressive loss of the visual field [1]. Secondary glaucoma develops in approximately 10–20% of patients with uveitis [2]. In the case of chronic, severe forms of inflammation, however, the incidence is higher and may reach as high as 46% [3]. The incidence of secondary glaucoma may also differ in the various different types of uveitis. It most commonly accompanies herpes simplex keratouveitis (54%), herpes zoster uveitis (38%), sarcoidosis (34%), Fuchs heterochromic iridocyclitis (27%), and uveitis associated with juvenile idiopathic arthritis (JIA) (15–35%) [4].
Ocular inflammation causes structural changes in the chamber angle, which lead to an elevation of IOP and subsequently to glaucoma neuropathy. The mechanisms by which uveitis leads to an elevation of IOP are an accumulation of inflammatory elements in the intertrabecular spaces, edema of the lamellas or angle closure as a consequence of swelling of the ciliary body. These changes mostly occur acutely and are reversible, in contrast with the formation of scars, anterior synechiae or growth of membranes in the chamber angle, which constitute chronic changes [3]. Another factor in the development of secondary uveitis glaucoma is the steroid component. It is important to differentiate between the steroid and inflammatory component of uveitic glaucoma; nevertheless, differential diagnostics may be complicated. The treatment of secondary uveitic glaucoma is commenced with local anti-glaucomatous agents, and it is also essential to suppress the inflammatory activity of uveitis by means of appropriate therapy. In a range of cases, conservative anti-glaucomatous therapy is ineffective, and it is therefore necessary to proceed to timely anti-glaucomatous surgery, or potentially also laser therapy. Filtration procedures are less successful in primary open-angle glaucoma. Repeated episodes of inflammation, the multiple mechanism of origin of glaucoma and complications in connection with uveitis make the surgical treatment of uveitic glaucoma a demanding procedure [4].
PATHOGENESIS OF SECONDARY UVEITIC GLAUCOMA
As yet, the detailed mechanisms of the development of secondary uveitic glaucoma have not been entirely clarified. However, elevation of IOP is in large part caused by an increase in the resistance of drainage pathways, leading to an imbalance between the production and drainage of the chamber fluid. This takes place in particular in the case of herpetic and chronic forms of uveitis. Paradoxically, during the activity of acute serofibrinous uveitis, IOP is frequently reduced as a consequence of the decrease of production of chamber fluid accompanied with an increase of uveoscleral drainage, and elevation of IOP may then occur only after pacification of the inflammation [1,3,5]. The aetiology can be divided into two large groups – inflammatory (in which the development of open-angle or angle-closure glaucoma results), and steroid-induced (Fig. 1).

1. Secondary open-angle glaucoma
When inflammation occurs, there is a breach of the blood-ocular barrier and a penetration of inflammatory cells into the anterior chamber, which subsequently congest the trabeculum. In addition, by means of producing pro-inflammatory cytokines, enzymes and free oxygen radicals, they cause swelling of the trabeculum and cytotoxic damage to the endothelial cells, and in the final result also scarring of the structures of the chamber angle [3,6], which leads to increased resistance in the drainage pathways and elevation of IOP. Upon activity of inflammation, there is an increased concentration of proteins in the chamber fluid, which on one hand congest the trabeculum and Schlemm’s canal, and also increase the viscosity of the anterior chamber fluid, thereby further contributing to the impediment of its drainage by the conventional pathway [1,5]. For example, in the case of chronic anterior uveitis, flare (turbidity) is a predictive factor of the development of secondary steroid-induced glaucoma [5]. Last but not least, direct inflammation of the trabeculum may result – trabeculitis – despite low inflammatory activity in the anterior chamber, as applies for example in the case of Posner-Schlossman syndrome, which has recently been attributed to infection by herpetic viruses (in particular cytomegalovirus) [5,7].
2. Secondary angle-closure glaucoma
Inflammatory cells and proteins in the anterior chamber fluid can lead to the creation of adhesions between the iris and the lens, and thereby cause a pupillary block. This condition is generally associated with chronic inflammation that is unresponsive to treatment. Pupillary block may be relative, in which the flow of the chamber fluid from the posterior to the anterior chamber is merely retarded (e.g. in the case of acute exacerbation of inflammation and the presence of fibrin), or absolute, upon complete seclusion of the pupil. The presence of posterior synechiae is considered to be a sign of severe chronic uveitis, and is associated with a high risk of the development of secondary glaucoma [5]. The formation of peripheral anterior synechiae (PAS) also occurs, especially in the lower part of the angle, where the largest accumulation of inflammatory cells and cellular detritus takes place. PAS exceeding the range of 180° develops in only 7% of eyes [5,8]. Factors predisposing patients to the development of PAS are a narrow angle or previous closure of the angle, pupillary block and front-to-back shift of the lens-iris diaphragm [5]. The formation of neovascularisations may occur in the angle, with fibrovascular closure [3]. In rare cases, closure of the angle may be the consequence of edema and anterior rotation of the ciliary body, for example in Vogt-Koyanagi-Harada syndrome [4].
3. Steroid-induced glaucoma
Local and systemic corticosteroids used in the treatment of uveitis inhibit the capacity of phagocytosis of the endothelial cells of the trabeculum, and thereby potentiate the congestion of the trabeculum with inflammatory cells and detritus. In addition, they stabilise the lysosomal membrane – this process leads to an accumulation of glycosaminoglycans in the cells, as well as to edema of the trabeculum and a further increase of the resistance in the drainage pathways [9]. In 18–36% of patients with uveitis, a contribution to the elevation of IOP is made precisely by these effects of corticosteroids. As a rule, secondary steroid-induced glaucoma develops within 5 weeks of the commencement of therapy. However, it may develop at any time, and it is not a simple matter to differentiate the adverse effects of the corticosteroids and the proportion of inflammation in the elevation of IOP [1,9]. The frequency of secondary steroid-induced glaucoma in the ordinary population is only 5% [1].
THERAPY OF SECONDARY UVEITIC GLAUCOMA
Therapy of secondary uveitic glaucoma is targeted at controlling intraocular pressure, treatment of any applicable systemic pathology and the reduction of IOP.
1. Treatment of inflammation
In the therapy of uveitis, it is always important to identify its potential correlation with a systemic pathology, and to introduce targeted therapy accordingly. It is essential to ensure interdisciplinary co-operation, with the aim of suppressing the inflammatory activity of uveitis and stabilising the systemic pathology. It has been demonstrated that the frequency of recurrences of the disease is directly proportionate to the affliction of the patient’s visual acuity [10].
a. Infectious uveitis
Elevation of IOP is especially linked to forms of uveitis with a herpetic aetiology, in which the initial elevation of IOP is pathognomonic. General therapy incorporates virostatics – aciclovir or valaciclovir. In the case of keratouveitis, ganciclovir or aciclovir can be administered locally. If the cornea is intact, treatment with local corticosteroids is fully indicated for infectious forms of uveitis, and frequently leads to a rapid reduction of IOP.
b. Immune-mediated and idiopathic uveitis
The therapy of immune-mediated uveitis in particular incorporates the administration of corticosteroids locally and generally, immunosuppressants and biological therapy.
Corticosteroids
Corticosteroids are the pharmaceuticals of first choice in the treatment of immune-mediated forms of uveitis. They are administered locally (topically, subconjunctivally, parabulbarly, intravitreally), and in the case of intermediate uveitis, posterior uveitis and panuveitis, or the necessity of treating a general underlying pathology, also systemically. Local corticosteroids are essential for the pacification of the inflammatory activity of anterior uveitis. Due to the potential risks in connection with their administration (secondary glaucoma, development of cataract etc.), it is necessary to consider any applicable long-term application carefully. In general, it applies that upon relatively short-term use in cases of acute serofibrinous anterior forms of uveitis, it is advantageous to use stronger corticosteroids (dexamethasone), and upon an elevation of IOP to add anti-glaucomatous agents. In cases of chronic anterior forms of uveitis, it is then necessary to consider the application of weaker corticosteroids (fluorometholone) upon an elevation of IOP.
Corticosteroids administered generally have a more rapid onset and are effective. However, they should not be administered long-term in higher doses [5].
Mydriatics and cycloplegics
Mydriatics and cycloplegics are indicated in the case of activity of inflammation, for preventing the formation of posterior synechiae and the growth of existing synechiae. Another reason they are prescribed is for pain relief [4].
Immunosuppressants
Antimetabolites (methotrexate, mycophenolate mofetil, azathioprine) and T-cell inhibitors (cyclosporine A, tacrolimus) are used if the pathology is resistant to treatment with corticosteroids or if there are severe contraindications for the administration of corticosteroids. As a rule, the onset of the effect takes place after a number of weeks, and treatment must be entrusted to an experienced doctor [17].
Biological therapy
In recent years there has been an expansion of the use of biological drugs, which have made a significant contribution to improving the prognosis of patients with autoimmune uveitis. This group of pharmaceuticals includes monoclonal antibodies against tumour necrosis factor alpha (adalimumab, infliximab ad.). Their effect has also been demonstrated for example in anti CD20 (rituximab), anti IL-6 (tocilizumab), anti IL-17 (secukinumab), anti IL-12 and IL-23 (ustekinumab). However, with the exception of adalimumab these pharmaceuticals have not been approved for the treatment of uveitis, and are used in an off-label regime [17].
2. Treatment of glaucoma itself
a. Medicamentous therapy
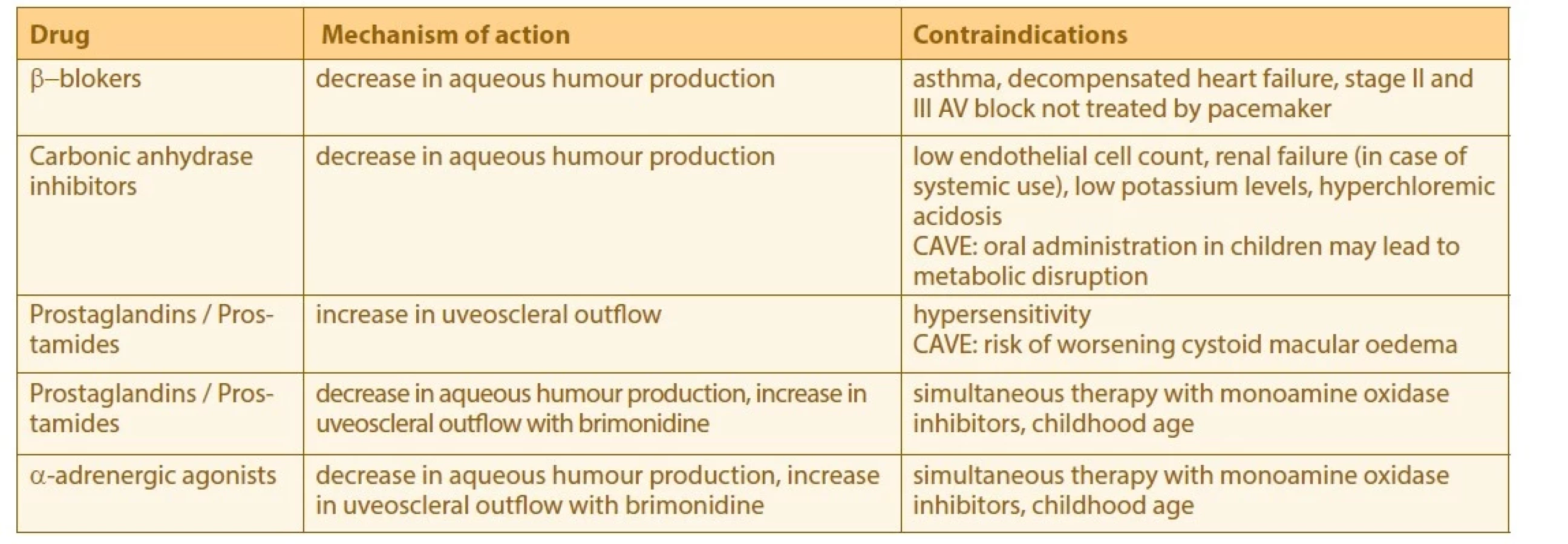
Therapy of secondary uveitic glaucoma is always commenced with local anti-glaucomatous therapy. The pharmaceuticals of first choice here are β-blockers and carboanhydrase inhibitors. However, in the case of systemic application of carboanhydrase inhibitors for patients in childhood age, caution is essential due to the risk of metabolic disorders. With prostaglandins there is theoretically a risk of a pro-inflammatory effect. However, on the basis of the data from the literature [11,12] this concerns a highly effective group of pharmaceuticals which are safe also for intraocular inflammations, which is also confirmed by our own experiences from clinical practice. α-adrenergic agonists can also be used, and have proven to be effective especially in combination with other anti-glaucomatous agents (Table 1). Miotics increase the risk of formation of posterior synechiae, in addition to which they have a pro-inflammatory effect and disrupt the blood-ocular barrier, and as a result they are contraindicated.
Hyperosmotic drugs increase the osmolarity of plasma and the extracellular spaces, with a subsequent increase in the export of water molecules from the cells to the blood vessels, and by this mechanism reduce IOP. They can be used in acute states for a rapid reduction of IOP, but long-term use is inadmissible.
b. Surgical therapy
Medicamentous therapy fails when administered for secondary uveitic glaucoma to a greater extent than in the case of primary open-angle glaucoma. In the case of persistent elevation of IOP despite the maximum tolerated anti-glaucomatous therapy, or in the case of pupillary block, it is appropriate to proceed to surgical therapy. Good perioperative control of the inflammatory process is of key importance for the success of surgical interventions. The choice of the specific approach depends on the experience of the operating surgeon, the clinical picture and previously performed procedures.
Surgical iridectomy and synechiolysis
Surgical iridectomy is indicated as the treatment of first choice in the case of pupillary block and angle closure. It is recommended that iridectomy is combined with synechiolysis. This treatment should disrupt not only posterior synechiae between the iris and the anterior surface of the lens, but also PAS [5].
Trabeculectomy
Trabeculectomy (TE) with the use of antimetabolites (mitomycin C, 5-fluorouracil) is the gold standard in the treatment of refractory uveitic glaucoma. Effective control of inflammation is of key importance for the success of the operation. In the ideal case, the finding in the eye should be without signs of activity of intraocular inflammation three months before the procedure. However, it is frequently not possible to abide by this recommendation due to pronounced elevation of IOP and the risk of progression of glaucoma neuropathy [5]. The success rate of TE reaches 54% after 5 years. However, 78% of patients have to use local anti-glaucomatous agents [1]. Patients with uveitis are also susceptible to a higher risk of postoperative hypotonia and a higher risk of scarring than patients with primary glaucoma [1,6].
Non-penetrative procedures – Deep sclerectomy
Deep sclerectomy with the use of antimetabolites has proven to be an effective surgical technique in the therapy of secondary uveitic glaucoma. However, after a certain time a significant number of patients require therapy with anti-glaucomatous agents, goniopuncture or other surgical procedure [13].
Drainage implants
Drainage implants of the type Ahmed, Baerveldt and Molteno have proven to be a very effective alternative, with a high success rate especially in eyes that have undergone previous procedures [1]. In the case of secondary glaucoma associate with JIA uveitis, they are recommended as the method of first choice [5]. Postoperative complications include decompensation of the cornea, diplopia or exposure of the implant. The risk of postoperative hypotonia is slightly higher than in patients with primary glaucoma, though the risk is not statistically significant. The success rate of the treatment is comparable with the success rate in the case of primary glaucoma [14,15].
Goniotomy
Goniotomy can be indicated as a safe alternative to TE for young patients and patients in childhood age, with a relatively high success rate [3,6].
Minimally invasive surgical procedures
In recent years there has been a development of methods of minimally invasive glaucoma surgery (MIGS) as safer alternatives to classic filtration procedures. These surgical interventions involve a minimal disruption of the normal anatomy of the eye. Micro-implants implanted ab interno or ab externo are used for the purpose of reinforcing existing drainage mechanisms (e.g. Preserflo, Xen, iStent, Trabectome etc.). However, there is not yet a sufficient quantity of data in order to assess the effect of MIGS on secondary uveitic glaucoma [6].
c. Laser therapy
The performance of laser iridotomy (LI) is effective in the case of treatment of pupillary block and angle closure. However, in the case of uveitic glaucoma, surgical iridectomy is frequently chosen due to the high risk of early failure of LI [18]. Selective laser trabeculoplasty (SLT) is not generally recommended for secondary uveitic glaucoma. However, in 2021 a study was published highlighting a similar effect of SLT in comparison with primary glaucoma. The degree of complications and failure was also comparable. Patients with a steroid component of secondary uveitic glaucoma especially benefited from SLT [16]. In the case of failure of surgical therapy, it is possible to select the method of transscleral cyclophotocoagulation, though it is necessary to exercise caution here. In the case of secondary glaucoma, this procedure brings with it the risk of development of hypotonia, deterioration to loss of sight, phthisis of the eyeball and exacerbation of inflammation in comparison with glaucoma of a different aetiology. For this reason, this option is one of the last used modalities following the failure of previous therapy [4,5].
CONCLUSION
Secondary uveitic glaucoma is a serious and sight-threatening complication of uveitis, the treatment of which may be demanding. Even despite the substantial development of the possibilities of therapy of primary glaucoma, in the case of secondary uveitic glaucoma there is still an absence of an extensive prospective randomised trial for comparison of the effectiveness of the various different methods. In comparison with primary glaucoma, medicamentous therapy fails more frequently, while surgical procedures may involve a higher risk of complications. Surgical therapy is strictly individual, and depends on the clinical picture, previous procedures undergone by the patient and the experience and preferences of the operating surgeon. Good control of the inflammation in the perioperative and postoperative period is of key importance. The authors of the study declare that no conflict of interests exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company. The study has not been printed elsewhere or submitted to any other journal, with the exception of congress abstracts and recommended procedures.
Received: August 17, 2022
Accepted: January 2, 2023
Available on-line: February 20, 2023
MUDr. Eva Škrlová
Oční klinika, 1. LF UK a VFN v Praze
Šejbalové 888/8
152 00 Praha 5
E-mail: eva@skrla.cz
Sources
1. Kalogeropoulos D, Sung VC. Pathogenesis of Uveitic Glaucoma. J Curr Glaucoma Pract. 2018;12(3):125-138.
2. Sayed MS, Lee RK. Current management approaches for uveitic glaucoma. Int Ophthalmol Clin. 2015;55(3):141-160.
3. Bodh SA, Kumar V, Raina UK, Ghosh B, Thakar M. Inflammatory glaucoma. Oman J Ophthalmol. 2011;4(1):3-9.
4. Muñoz-Negrete FJ, Moreno-Montañés J, Hernández-Martínez P, Rebolleda G. Current Approach in the Diagnosis and Management of Uveitic Glaucoma. Biomed Res Int. 2015;2015 : 742792.
5. Sng CC, Ang M, Barton K. Uveitis and glaucoma: new insights in the pathogenesis and treatment. Prog Brain Res. 2015;221 : 243-269.
6. Kalogeropoulos D, Kalogeropoulos C, Moschos MM, Sung V. The Management of Uveitic Glaucoma in Children. Turk J Ophthalmol. 2019;49(5):283-293.
7. Pleyer U, Chee SP. Current aspects on the management of viral uveitis in immunocompetent individuals. Clin Ophthalmol. 2015;9 : 1017-1028.
8. Sherman ER, Cafiero-Chin M. Overcoming diagnostic and treatment challenges in uveitic glaucoma. Clin Exp Optom. 2019;102(2):109-115.
9. Phulke S, Kaushik S, Kaur S, Pandav SS. Steroid-induced Glaucoma: An Avoidable Irreversible Blindness. J Curr Glaucoma Pract. 2017;11(2):67-72.
10. Dana MR, Merayo-Lloves J, Schaumberg DA, Foster CS. Prognosticators for visual outcome in sarcoid uveitis. Ophthalmology. 1996;103(11):1846-1853.
11. Taylor SR, Gurbaxani A, Sallam A, Lightman S. Topical prostaglandin analogues and conjunctival inflammation in uveitic glaucoma. Open Ophthalmol J. 2012;6 : 75-78.
12. Markomichelakis NN, Kostakou A, Halkiadakis I, Chalkidou S, Papakonstantinou D, Georgopoulos G. Efficacy and safety of latanoprost in eyes with uveitic glaucoma. Graefes Arch Clin Exp Ophthalmol. 2009;247(6):775-780.
13. Mercieca K, Steeples L, Anand N. Deep sclerectomy for uveitic glaucoma: long-term outcomes. Eye (Lond). 2017;31(7):1008-1019.
14. Ramdas WD, Pals J, Rothova A, Wolfs RCW. Efficacy of glaucoma drainage devices in uveitic glaucoma and a meta-analysis of the literature. Graefes Arch Clin Exp Ophthalmol. 2019;257(1):143 - 151.
15. Tan AN, Cornelissen MF, Webers CAB, Erckens RJ, Berendschot T, Beckers HJM. Outcomes of severe uveitic glaucoma treated with Baerveldt implant: can blindness be prevented? Acta Ophthalmol. 2018;96(1):24-30.
16. Zhou Y, Pruet CM, Fang C, Khanna CL. Selective laser trabeculoplasty in steroid-induced and uveitic glaucoma. Can J Ophthalmol. 2021.
17. Klímová A, Heissigerová J, Brichová M, Říhová E, Svozílková P. Léčba uveitid. Remedia 2018; 28 : 78-82. Czech.
18. Peter A. Netland, MD. PhD. Treating Uveitic Glaucoma: What Works? Review of Ophthalmology, 2018 Mar, available from: https://www. reviewofophthalmology.com/article/treating-uveitic-glaucoma-what-works
Labels
OphthalmologyArticle was published in
Czech and Slovak Ophthalmology

2023 Issue 3
Most read in this issue
- LASER THERAPY OF RETINAL TEARS
- CHANGES IN THE VISION OF ADULT AMBLYOPIC PATIENTS FOLLOWING CLEAR LENS EXTRACTION
- GIANT PROLACTINOMA. A CASE REPORT
- PATHOGENESIS AND CURRENT METHODS OF TREATMENT OF SECONDARY UVEITIC GLAUCOMA. A REVIEW