
Digital Eye Strain in a Population of Young Subjects
Authors:
P. Veselý 1,2; L. Hanák 1,2; P. Beneš 1,2
Authors‘ workplace:
Oddělení nemocí očních a optometrie, Fakultní nemocnice u svaté Anny, Pekařská 53, 65691 Brno. Přednosta: MUDr. Lubomír Hanák, MBA.
1; Katedra optometrie a ortoptiky, Lékařská fakulta, Masarykova univerzita, Kamenice 5, 62500 Brno. Přednosta: Mgr. Pavel Beneš, Ph. D.
2
Published in:
Čes. a slov. Oftal., 74, 2018, No. 4, p. 154-157
Category:
Original Article
doi:
https://doi.org/10.31348/2018/1/5-4-2018
Overview
The main goal of our study was to prove short-term objective influence of near addition and relieving prism on accommodative and vergence facility in group of young healthy persons. Further, we wanted to prove objective and subjective difference between two types of soft contact lenses during working with digital device.
We had in total 37 subjects in our study. The first group contained 37 subjects with average age 23 years without important eye pathology. The second group contained 8 subjects with the same average age without important eye pathology. In the first group of subjects, we measured binocular accommodative facility (BAF) and binocular vergence facility (BVF) with and without addition 1 D and with and without relieving prism 2 pD BO at working distance 45 cm. In the second group, we evaluated BAF, BVF and standardized questionnaire (Computer Vision Syndrome Questionnaire – CVS-Q, Sequí M. 2015) during usage of two types of soft contact lenses. The first type of contact lenses (type 1) contained relieving prism for PC working and type 2 was soft contact lens with aspheric design.
In the first group of subjects, we measured these values: BAF without addition = 12.78 cpm, BAF with addition = 11.57 cpm, BVF without prism = 12.32 cpm, BVF with prism = 11.59 cpm. In the second group of subjects, we measured with contact lens type 1 these values: BAF = 12.13 cpm, BVF = 13.63 cpm and questionnaire score 9.43 points. With contact lens type 2 we measured BAF = 11.75 cpm, BVF = 11.63 cpm and questionnaire score 12.86 points. We proved statistically important different between two variable only in the first group between BAF with and without addition and BVF with and without relieving prism.
In conclusion, we found statistically important decrease in variable BAF and BVF with usage of addition and relieving prism. We found that neither addition nor prism have positive influence on increase of BAF and BVF. Subjects in second group had higher BAF and BVF values with both types of contact lenses in comparison with natural values. We found that with contact lens type 1 (with addition) subjects had higher BAF and BVF values in comparison with contact lens type 2 (aspheric). Subjects with contact lens type 1 had also lower (better) questionnaire score, i.e. 9.43 versus 12.86 point.
Key words:
Digital eyestrain syndrome, accommodative and vergence facility, addition, relieving prism.
INTRODUCTION
Upon work with a digital device (e.g. mobile telephone, tablet or personal computer), an increased strain is placed on the accommodative and vergence facility. This may be manifested in both subjective and objective complaints. We may include among subjective complaints such phenomena as stinging of the eyes, asthenopia (eye strain), blurred vision or double vision. Objective complaints may include for example transitory heterotropia or heterophoria. These complaints may also appear in individuals with normal binocular vision. Individuals with inadequate correction of a refractive error or a defect of simple binocular vision are naturally more afflicted. This issue is dealt with for example by our previous study (10).
In optometry we can evaluate simple binocular vision with the aid of objective tests or with the aid of questionnaires. In the case of accommodation, besides its amplitude or relative accommodation, we are interested also in the value of the “accommodative facility” or the ability to adjust accommodation to a specific working distance. Measurement is conducted with the aid of special spherical flippers (Fig. 1), where the application of converging and diverging spherical glasses lenses is alternated. We can perform this measurement for monocular accommodative vision (MAV) or for binocular accommodative vision (BAV). The normal values of MAV and BAV reach over 10 cycles per minute (cpm). If we find a reduced BAV value while the MAV value is normal, this probably concerns a vergence problem.
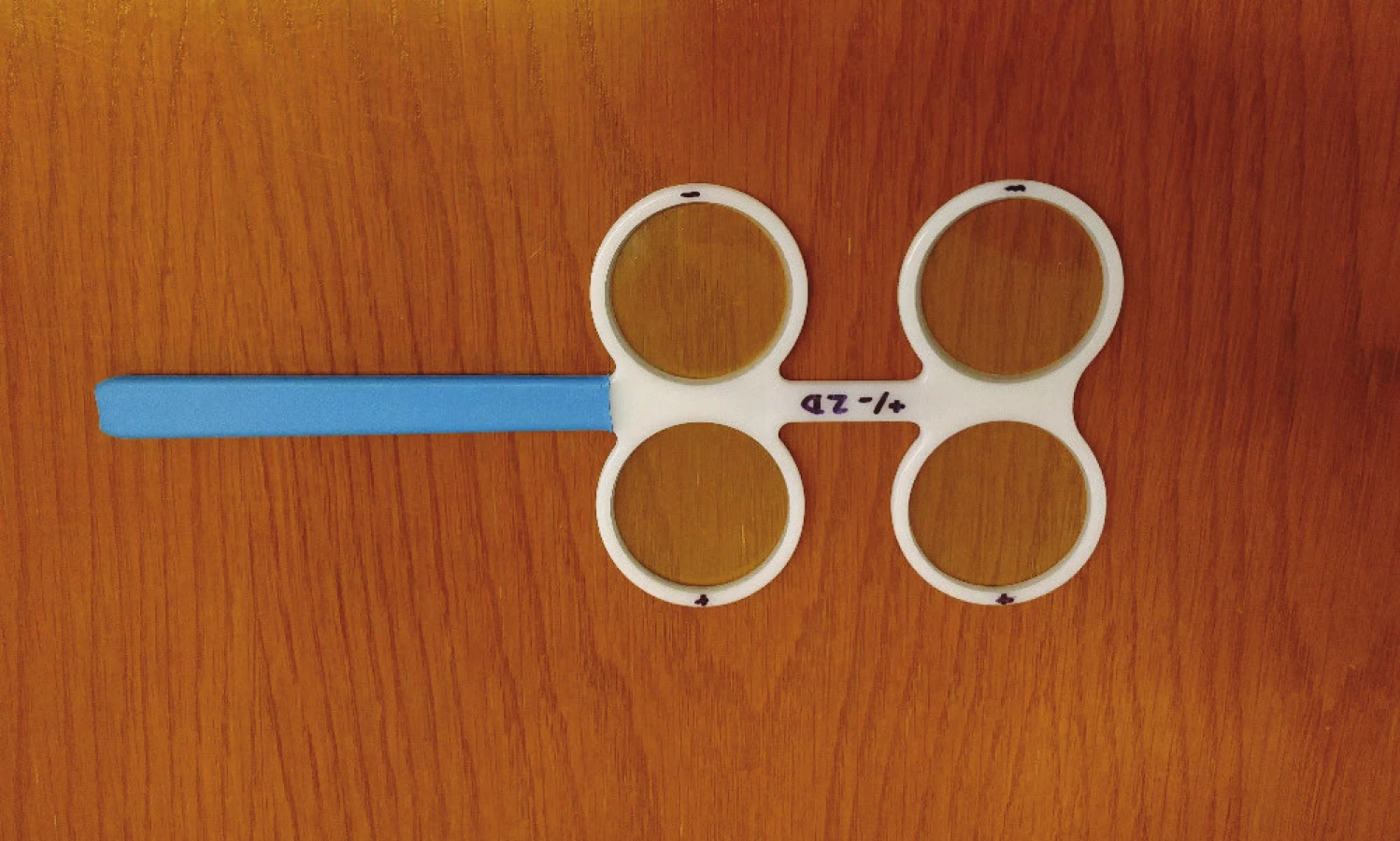
Similarly, we can evaluate the vergence capacity of the binocular apparatus not only on the basis of the absolute value of fusion vergences (fusion widths), but also on the basis of “binocular vergence facility” (BVF). This measurement is usually performed with a prismatic flipper (Fig. 2), where the application of prisms with an outward and inward base is alternated.

In patients with an inadequately corrected refractive error, defect of simple binocular vision or individuals who place an excessive strain on their binocular apparatus, there is a temporary reduction of certain parameters of simple binocular vision. These are adaptive changes which we must separate from pathological changes (e.g. ocular manifestations of myasthenia gravis) and physiological changes (e.g. presbyopia). For example, in some studies (1, 8) a reduction of relative accommodation, fusion vergence or accommodative and vergence facility has been demonstrated.
At present special optic aids are available on the market which have the role of reducing accommodative stress and thus ensuring comfortable work with a digital device. In the case of glasses lenses these are special monofocal glasses lenses with a progressive design and low addition (0.5 to 0.8 D). Furthermore they may also contain a surface anti-reflection finish, reducing reflection of short-wave blue light, or special absorption compounds which are incorporated into the monomer of the future glasses lens for the same reason.
In the case of soft contact lenses, this primarily concerns lenses which thanks to their aspherical design reduce the spherical defect of the eye, or behave like a lens with a progressive design with low addition.
The aim of our study was to verify the positive influence of glasses addition and a relieving prism on certain parameters of binocular vision (BAF and BVF), and at the same time to verify the positive influence of aspherical design of soft contact lenses for individuals working with a digital device.
METHOD
In our study we had a total of 37 ametropic or emmetropic probands available to us in the first group, with an average age of 23 years (SD 1.5). In the second group we had 8 emmetropic probands with an average age of 23 years (SD 0.92). In the first group there were 8 male individuals, the remaining probands were female.
A precondition for our measurement was the presence of current full binocular glasses correction and the absence of a serious defect of simple binocular vision, such as blunt-sightedness or strabismus. There was no serious ocular or general pathology in our tested probands at the given time.
We first of all measured the probands in the first group for their accommodative (BAF) or vergence facility (BVF) with the aid of a spherical (+/-2D) or prismatic flipper (3p D BO/BI). We subsequently measured BAF after binocular application of addition of 1 D and BVF with a binocular relieving prism of 1 pD placed with the base outward bilaterally (total 2 pD BO). During the examination the probands with acute glasses spherical-cylindrical correction watched a separate optotype symbol at a distance of 45 cm. The order of testing procedures was alternated in the middle of the tested cohort in order to exclude the possibility of adaptation to the used examination methods.
In the case of the probands from the second group, after application of the first type of contact lens (type 1 = sphere -0.25 D with relieving addition), we measured BAF and BVF, again upon fixation of a separate optotype symbol at a distance of 45 cm. After a week of use of these lenses (especially upon work with a digital device) we submitted a questionnaire to the probands (Computer Vision Syndrome Questionaire CVS-Q (4)). We repeated the procedure with the second type of contact lens (type 2 = sphere -0.25 D with aspherical design). The individual probands did not know which type of contact lenses they were using during the course of wearing. The material of both types of contact lenses was silicon-hydrogel. The trial was single-blind.
The results of the measurement were converted into an MS Excel table, and subsequently statistically evaluated with the aid of the statistical program Statistica version 12 from the STATSOFT company and MedCalc. The selected level of statistical significance was p=0.05.
RESULTS
In the first group of probands we measured the following values: binocular accommodative facility BAF without addition = 12.78 cpm, binocular accommodative facility BAF with addition = 1.57 cpm, binocular vergence facility BVF without prism = 12.32 cpm and binocular vergence facility BVF with prism 11.59 cpm. On the level of statistical significance of p=0.05 we demonstrated a statistically significant difference between BAF values without and with addition and BVF without and with a prism (Graph 1 and 2).


In the second group of probands, with a type 1 contact lens we measured values of BAF = 12.13 cpm, BVF = 13.63 cpm and questionnaire score of 9.43 points (Graph 3). With a type 2 contact lens we measured values of BAF = 11.75 cpm, BVF = 11.63 cpm, questionnaire score of 12.86 points (Graph 4 and 5).



DISCUSSION
Digital eye strain or Computer Vision Syndrome (CVS) is a temporary condition of vision which occurs following long-term exertion of the eyes during work on a computer (6). Problems in CVS are caused primarily by excessive stress on the ocular muscles or unnatural body posture. The solution to these complaints is a multi-disciplinary task, which involves not only the field of ophthalmology and optometry, but also for example ergonomics, and occupational safety and hygiene.
In our study we focused on verifying two hypotheses. In the case of the first hypothesis we wished to demonstrate the positive influence of addition and a relieving prism on close-up work with the aid of measuring binocular accommodative (BAF) and binocular vergence facility (BVF). Here we demonstrated that upon the application of addition there is a statistically significant reduction of BAF, and similarly upon the application of a relieving prism (total 2 pD BO) there is a statistically significant reduction of BVF. We may therefore deduce from our results that neither addition or a relieving prism contribute to a short-term increase of comfort upon close-up work. The long-term effect of these elements has not been investigated in our study.
Rosenfield (2) in his study examined certain parameters of binocular vision and CVS. In his probands he measured monocular (MAF) and binocular accommodative facility (BAF) before and after 25 minutes of work with a personal computer. The results did not demonstrate statistical differences between the values of MAF and BAF before and after the test.
The second hypothesis was focused on demonstrating an improvement of accommodative and vergence performance in the case of two types of modern soft contact lens. The first type (type 1) of contact lens, thanks to its aspherical design, contains low addition for near vision (0.5 D) and the second type (type 2) is “merely” aspherical. This type therefore corrects the spherical error of display that the average human eye usually manifests. For example, according to the study by Smith et al. (5), this concerns a value of 0.005134 µm/mm4 for the whole eye. This value of spherical aberration of the whole eye is composed of positive spherical aberration of the cornea (0.032214 µm/mm4) and negative spherical aberration of the ocular lens (-0.012017 µm/mm4). Simply speaking, we can therefore say that in the case of a multifocal contact lens the aim is to add addition, increase the spherical aberration of the eye and therefore increase the depth of acuity at the expense of quality of the image. In the case of an aspherical contact lens the main aim is the precise opposite, namely to correct the spherical aberration of the eye in order to reduce the depth of acuity and increase the quality of the image (9).
Previous studies show that upon wearing soft contact lenses, there is a statistically greater incidence of CVS (65% v 50%, p=0.02) than in persons who do not use these lenses (7).
Our results demonstrated that in the case of both types of contact lenses there was an increase in BAF and BVF as against the values of BAF and BVF that we measured without correction with contact lenses. Higher values of BAF and BVF were attained with type 1. This result is therefore probably influenced by the addition of the given contact lens. At the end of each weekly period of wearing contact lenses, the probands completed a special questionnaire (CVS-Q), which demonstrated a lower (better) score for the first type of contact lens. However, the resulting difference is not statistically significant.
In the first case (type 1), a total of 9.43 points was scored in the CVS-Q questionnaire. In the second case (type 2) the score was 12.86 points. In both cases the limit (6 points) according to which digital eye strain occurs was exceeded.
CONCLUSION
In our study we tested certain parameters of simple binocular vision in probands from two groups. The first group comprised 37 probands with an average age of 23 years. In these probands we demonstrated a statistically significant reduction of BAF and BVF upon the use of addition of 1 D or a relieving prism of total 2 pD with base outward. Our results are in accordance with other studies which have not demonstrated the influence of work on a computer on certain parameters of simple binocular vision (e.g. BAF).
In the second group, which comprised 8 probands with an average age of 23 years without refractive error and ocular pathologies, we examined the function of two types of soft contact lens. Type 1 was with addition of 0.5 D and type 2 was a lens with an aspherical design, correcting spherical defect of the eye. The results demonstrated an increase of BAF and BVF in comparison with natural values. In conclusion we evaluated the results of the CVS-Q questionnaire and determined a better result (lower score) for type 1 contact lenses. However, the resulting score may also have been influenced not only by the optical design of the contact lenses, but also by the properties of the materials from which the contact lenses were produced.
The authors of the study declare that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
This study originated within the framework of a specific research project of the rector MUNI/A/0749/2017.
Received: 13. 6. 2018
Accepted: 30. 8. 2018
Available on-line: 18.3.2019
Mgr. Petr Veselý, DiS., Ph.D.
Oddělení nemocí očních a optometrie
Fakultní nemocnice u sv. Anny
Pekařská 53, 656 91 Brno
e-mail: petr.vesely@fnusa.cz
Sources
1. Allen, PM., O´Leary, DJ.: Accommodation functions: Co-dependency and relationship to refractive error. Vision Res, 46; 2006 : 491-505.
2. Rosenfield, M.: Computer vision syndrome: a review of ocular causes and potential treatments. Opthalmic Physiol Opt, 31; 2011 : 502-515.
3. Rozsíval, P. a kol.: Oční lékařství. Praha: Galén, 2006. 363 s. ISBN 80-7262404-0.
4. Seguí del Mar, M., Cabrero-García, J., Crespo, A. et al.: A reliable and valid questionnaire was developer to measure Computer Vision Syndrome at the workplace. J Clin Epidemiol, 2015, doi: 10.1016.
5. Smith, G., Cox, JM., Claver, R. et al.: The sperical aberration of the crystalline lens of the human eye. Vision Res, 41; 2001 : 235-243.
6. Syndrom počítačového vidění (CSV) [online]. Wikipedia, 2017 [cit. 2018-03-21]. Dostupné z: https://cs.wikipedia.org/wiki/Syndrom_po%C4%8D%C3%ADta%C4%8Dov%C3%A9ho_vid%C4%9Bn%C3%AD.
7. Tauste, A., Ronda, E., Molina, MJ. et al.: Effect of contact lens use on Computer Vision Syndrome. Ophthalmic and Physiological Optics, 36; 2016 : 112-119.
8. Tosha, C., Borsting, E., Ridder III, WH. et al.: Accommodation response and visual discomfort. Ophthalmic Physiol Opt, 29; 2009 : 625-633.
9. Trusit D. Understanding multifocals and getting them to work. Optician, 249; 2015 : 12-17.
10. Veselý, P., Spurná, G., Hanák, L. et al.: Poruchy jednoduchého binokulárního vidění u heteroforií a jejich řešení brýlovou korekcí. Cesk Slov Oftalmol, 72; 2016 : 223-225.
Labels
OphthalmologyArticle was published in
Czech and Slovak Ophthalmology

2018 Issue 4
Most read in this issue
- Vertical Strabismus – Indication of Surgical Techniques on the Inferior Rectus Muscle
- Keratopigmentation (Corneal Tattoo) – Our First Experience
- Diagnosis of Familial Hypercholesterolaemia on First Sight? The Role of the Ophthalmologist in Identifying Patients with Familial Hypercholesterolaemia
- Correction of Myopia and Myopic Astigmatism by Implantation of a Phakic Posterior Chamber Implantable Collamer Lens