
Health literacy on HIV infection among adolescents in the Czech Republic: a case study of two Czech cities Plzeň and České Budějovice
Zdravotní gramotnost týkající se infekce HIV mezi adolescenty v České republice: případová studie ze dvou českých měst – Plzně a Českých Budějovic
Zdravotní gramotnost je důležitým předpokladem pro udržení zdravé populace. V České republice a mezi českými autory neexistuje mnoho studií zaměřených na zdravotní gramotnost týkající se infekce HIV ve skupině dospívajících osob. V kontrastu s tím stojí poměrně vysoký vědecký zájem o informovanost a vnímání této problematiky dospívajícími v nejvíce postižených oblastech světa, zejména v subsaharské Africe a Indii.
Dospívající patří v oblasti infekce HIV do vysoce rizikové skupiny, přičemž vzdělání je jedním z hlavních faktorů ovlivňujících úroveň rizika infekce HIV. Zvyšování zdravotní gramotnosti je však realizováno pouze na některých typech středních škol.
Cílem této studie je ověřit zdravotní gramotnost týkající se infekce HIV u adolescentů ve dvou typech středních škol (gymnáziích a středních odborných učilišť), a to ve dvou krajských městech: v Plzni a v Českých Budějovicích.
Pro zjištění úrovně zdravotní gramotnosti v oblasti infekce HIV byl sestaven dotazník s 13 otevřenými a 9 uzavřenými otázkami, který byl implementován mezi studenty (N = 1 942) v 16 vybraných školách v roce 2015. Dotazník byl předem testován a jeho vyplnění zabralo cca 15 minut.
Studie prokázala, že ženy studující na gymnáziích disponují nejlepšími znalostmi v oblasti zdravotní gramotnosti infekce HIV. Oproti tomu nejnižší úroveň znalostí byla identifikována mezi muži, kteří studují střední odborná učiliště.
Znalosti a orientace v oblasti problematiky HIV/AIDS však nestačí. Důležitý je i fakt, zda dospívající dokáží tyto znalosti přeměnit ve svůj prospěch, a přispět tak k redukci rizika infekce HIV a svého vlastního rizikového chování.
Zavedení preventivních programů na všech typech škol a vzdělávání adolescentů v oblasti sexuálně přenosných nemocí je pro snížení expozice vůči HIV zcela zásadní. Existující rozdíly mezi pohlavími a školami mohou u některých těchto skupin zvýšit riziko infekce. Na základě zjištěných skutečností doporučujeme hledat cesty pro sjednocení a zefektivnění přístupu k výuce tohoto tématu na všech typech škol a více programy zaměřit na chlapce, neboť muži jsou největší skupinou HIV pozitivních osob v Česku.
Klíčová slova:
zdravotní gramotnost – deskriptivní průřezová studie – HIV/AIDS – studenti – Česká republika
Authors:
J. C. Sekera 1; J. Preis 2; P. Pazdiora 3
![]()
Authors‘ workplace:
Charles University, Faculty of Science, Prague, Czech Republic
1; The University of West Bohemia, Faculty of Economics, Pilsen, Czech Republic
2; Charles University, Faculty of Medicine in Pilsen, Czech Republic
3
Published in:
Epidemiol. Mikrobiol. Imunol. 69, 2020, č. 4, s. 182-188
Category:
Original Papers
Overview
Despite health literacy being an important assumption for maintaining a healthy population, there are not many studies focusing on health literacy concerning HIV infection among adolescents in the Czech Republic and among Czech authors. In contrast, there are plenty of scientific papers and researches focused on awareness and susceptibility of adolescents in most affected regions of the world, Sub-Saharan Africa and India particularly.
Adolescents belong to a high-risk group of the population. Education is one of the most important factors that influence the level of risk of HIV infection. However, increasing health literacy is only implemented in some types of secondary schools in the Czech Republic. The goal of this study is to verify health literacy concerning HIV infection among adolescents in two types of Czech secondary schools (grammar school and vocational school) in two Czech regional cities (Plzeň and České Budějovice).
To determine the level of health literacy of HIV infection, a questionnaire (13 open and 9 closed questions) was compiled. A descriptive cross-sectional study was implemented among students (N = 1 942) of 16 chosen schools in two cities of the Czech Republic in 2015. The questionnaire was pre-tested and it took about 15 minutes to complete. The association was tested by a chi-square test, the averages were then compared with an independent t-test, the p-value (0,05) was used in all tests.
Most of the students (67,3%) had good health literacy about HIV/AIDS, statistically significant differences were found between students of grammar schools and vocational schools (p = 0,012). Differences were also found between men and women (p = 0,037). The respondents showed the best knowledge about transmission (94,3%), the poorest about epidemiological questions (18,3%). Gender and the type of school had a statistically significant influence on the level of knowledge (gender x2; p = 0,042, types of a school x2; p = 0,031).
In this cross-sectional study, women studying at grammar schools had the best knowledge of HIV/AIDS. In contrast, the lowest level of knowledge was found in men studying in vocational schools. The school types and gender had a statistically significant influence on the level of knowledge. However – knowledge is not enough. To reduce infection risk potential will mean to help adolescents to transform knowledge into diminishing of their risky behaviour.
The implementation of prevention in all types of schools is crucial for the reduction of exposure from HIV infection. We consider educating adolescents about sexually transmitted diseases important. Despite that our research showed differences among schools and gender. Those differences can make a particular group be more at risk of being infected. Based on the findings, it would be suitable to unify and improve the approach to the education of this topic in all types of schools and to target preventive and educational techniques to boys more, since men are the biggest group of the HIV positive people in the Czech Republic.
Keywords:
health literacy – descriptive cross-sectional study – HIV/AIDS – students – Czech Republic
INTRODUCTION
HIV/AIDS knowledge is one of the basic attributes of prevention. Studies focused on the knowledge delivery are being implemented across the world, contain various sets of questions and they bring various results.
There is a similarity in the level of knowledge about three basic ways of the HIV transmissions in most of the studies: vertical (mother to child); sexual (particularly vaginal or anal intercourse); parenteral (other way, particularly via syringe). For example, in some secondary schools in Nigeria [2] it was ascertained that more than half of the students still believed a myth, that HIV can be transmitted by a mosquito bite.
Also, the level of knowledge depends on the family, Oljira et al., 2013 [15], found out that children that had a better family background had better knowledge. Othman’s, (2015) [16] results showed that boys had more knowledge than girls and he goes on to say that the higher the age, the better the knowledge; the type of school also plays a role. A lot of studies uncovered the fact that many respondents thought HIV can be cured, for example, Shiferaw et al., 2011 [21], Gao et al., 2012 [5].
Adolescents had good knowledge on the ways of transmission [17] and infection prevention [10] in the Czech Republic. This is in contrast to what some foreign literature suggests, that there is a problem between the level of knowledge about HIV and sexual behaviour in relation to infection [17], [26], [6] and attitudes towards HIV + people [10], [21], [1].
In 2007, Kirby, Larris, Rollery [7] published a paper that summarised data from 83 different studies. The authors tried to measure the effectiveness of programs focused on issues like HIV infection, STDs, pregnancy of adolescents and high-risk sexual behaviour as long as they were implemented directly into the curricula and how much they affected the behaviour of adolescents. The findings were very positive. Based on the authors’ research, high-quality programs bring important information and most importantly they help young people make informed decisions and lower their high-risk sexual behaviour.
In the Czech Republic, the first case of HIV infection was reported in 1985 [3]. By the end of 2018, 3 338 cases had been reported. Out of that, 2 524 were Czech citizens, 86% were men, the sexual way of transmission was the most common one especially for MSM (Men having sex with men) [18]. People aged 15–19 years (the age of secondary school students) were 2.6% of PLWHIV (People living with HIV) in 2018 [18]. Age-specific prevalence was 19.3 cases per 100 000 and age-specific incidence was 1.1 per 100 000 in 2017 [18].
The education system in the Czech Republic is conducted mainly in a formal context (provided by a system of state and private schools). The education system is based on the Strategy of Education Policy of the Czech Republic until 2020, which has been in force since 2014. The aim of the education system is to define basic approaches in education at all categorically similar schools throughout the Czech Republic. These curricular documents work on two levels. The Framework Educational Programs (FEPs) apply across the board and the School Educational Programs (SEPs) apply to individual schools. FEPs are precisely defined for each type of school (FEPs for primary education, grammar schools, secondary, vocational education). The FEP for grammar schools and secondary technical education (SOV) are further divided into categories and fields. FEPs should ensure uniform access to information across the Czech Republic.
HIV/AIDS are defined in the FEP for primary education (elementary schools). The HIV/AIDS issue is integrated into the area of ‘Health Care’ and is defined as ‘protection against transmissible blood infections (hepatitis, HIV/AIDS) [13].
The situation is, however, different in secondary education, where 3 types of schools belong to: grammar schools, high schools and vocational schools. FEP for vocational education does not contain any information about HIV/AIDS. The following topics are the closest ones: ‘Prevention of injuries, diseases and health risks’ and ‘Partnerships, human sexuality’ [12].
On the other hand, HIV/AIDS issues are integrated in grammar schools’ FEPs. This topic is dealt with in the subject ‘Health Education’ and the area of ‘health risks and their prevention’ [11], which also includes the issue of HIV/AIDS.
This study is focused on health literacy about HIV infection, which means knowledge, motivation and competence of people to obtain, understand, evaluate and apply relevant information about HIV infection in their lives and to help them to make relevant and good decisions.
The authors of this paper want to verify health literacy of HIV infection among adolescents in two types of secondary schools – grammar schools and vocational schools.
METHODS
A questionnaire was created to ascertain the level of knowledge of health literacy about HIV infection. It was focused on determining the level of knowledge related to HIV/AIDS and it consisted of three parts (biomedicine, epidemiology, behaviour) and demographic characteristics. The pre-testing of the questionnaire was done in a grammar school and vocational school which were not included in the analyses. It took 15 minutes to complete the questionnaire and it was done during the presence of teachers. Distribution of the paper version of the questionnaire was done personally along with introducing the project to the headmaster who then provided the completed questionnaires back, which was accompanied by his feedback. The questionnaire was anonymous which helped to make complications related to GDPR (General Data Protection Regulation) much easier, though GDPR was not implemented so strictly in the EU at the time of our research. Nine questions out of thirteen were closed and only one answer was always correct. Demographic questions were meant to find out the respondents’ age, gender, the school, and the year the students were in. The first set of question (biomedical) consisted of five questions focused on terminology and infection progress (e.g. stages of HIV infection names, explaining the difference between HIV and AIDS, examples of opportunistic infections associated with AIDS etc). The second set was focused on epidemiological know-ledge, it contained five questions about the epidemiology of HIV infection and its impact on society (e.g. discovery of AIDS, most affected countries in the world, number of positive people in the Czech Republic etc.). The last set (containing 3 behavioural questions) was focused on how it is transmitted and the source from which students get the information (e.g. transmission routes; where to look for the information how to protect against HIV; possible transmission routes for HIV infection; learning about HIV/AIDS at your school, etc).
It was possible to gain 19 points. Each question had a different importance. Each closed question could always be awarded only one point. In the case of an open question, it was possible to obtain more points – depending on the number of correct answers. The 13th question was not included in the total rating. It only provided information about data sources.
The questions were scored differently (see Table 2). All closed questions were for 1 point, open questions were scored according to the number of correct answers, e.g. if the respondent listed two correct opportunistic infections, he received two points. For a question on HIV transmission, a maximum of 3 points could be earned according to the three basic transmission routes. In the question of explaining HIV and AIDS, respondents received one point for each correct explanation of the concept, so they could receive a total of 2 points on this question.
The overall evaluation of health literacy about HIV was 0–5 poor, 6–12 acceptable and 13–19 very good.
The descriptive cross-sectional study was implemented in 2015 among students of 16 chosen secondary schools in two regional cities (Plzeň, České Budějovice), in the Czech Republic. The original plan was to carry out a survey in all grammar and vocational schools in these cities (20 schools altogether). The participation of schools was, however, voluntarily, and one grammar school in České Budějovice and three vocational schools in Plzeň rejected. Finally, the study was carried out at all grammar schools in Plzeň (5), at 5 out of 6 grammar schools in České Budějovice (CB) and at 6 out of 9 vocational schools in Plzeň. There was no vocational school in České Budějovice at the time of the study.
The obtained anonymous data was then analysed using the SPSS version 23 program. First, descriptive analysis of frequencies, proportions and averages was performed. The Chi-square test was used to test the association of the average score of points between categorical variables. P <0.05 was determined for statistical significance. To compare the average score of points (gender, city, type of school) a two-sample T-test was used, preceded by the F-test for variance conformity testing.
RESULTS
In total, 5 560 questionnaires were distributed, 2 105 were filled in (rate of return 37.9%). During the revision, the number was reduced to 1 942 respondents.
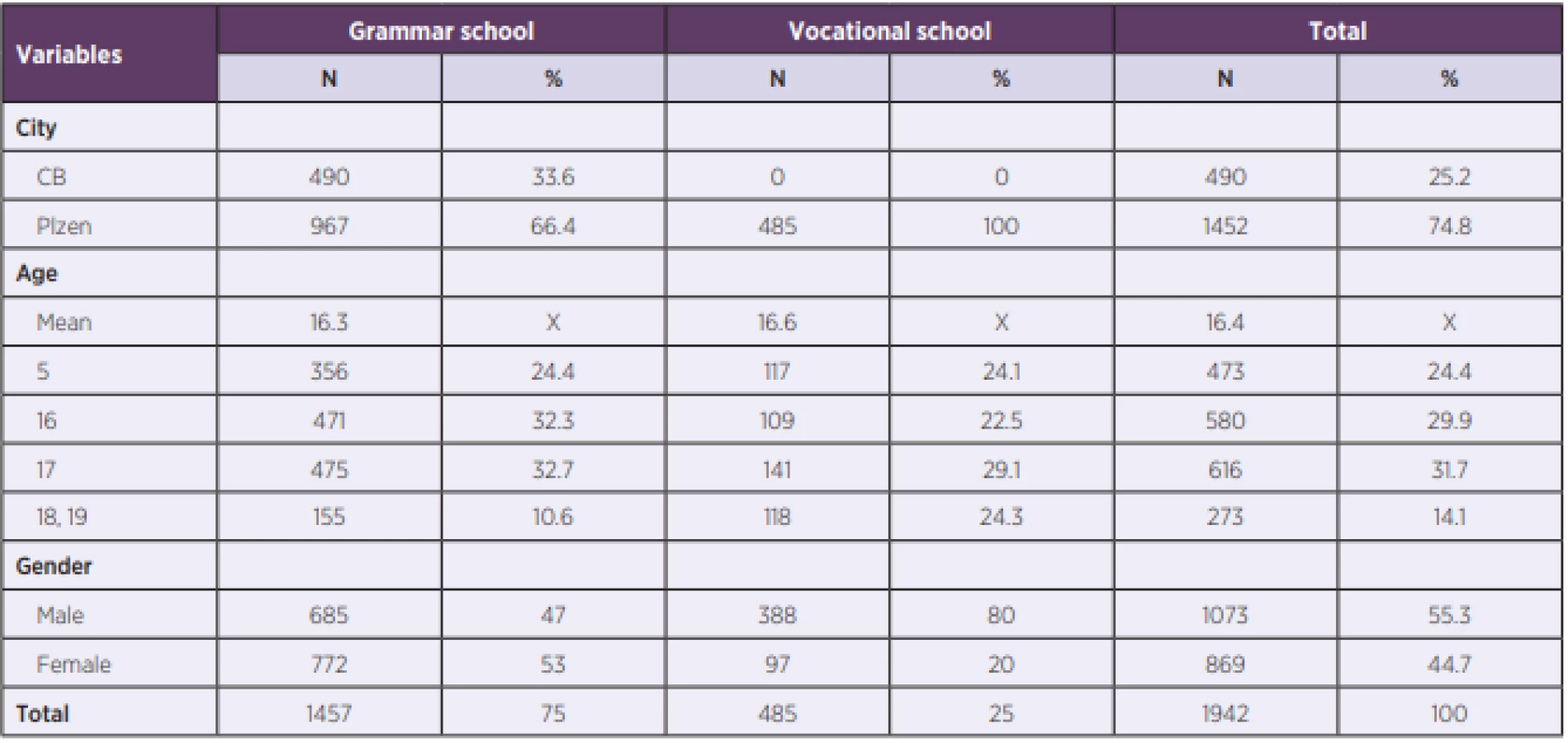
Out of 1 942 respondents, 55.3% were males. This occurrence was caused by the lower number of females in the vocational school (20%). The highest share of respondents from one school in total was 14.6 % and the lowest one was 2.2%. The respondents were from 15 to 19 years old, the average age was 16.4 years. The rest of the characteristics of the respondents are presented in Table 1.
The highest level of health literacy was demonstrated for HIV treatment and transmission. When asked about the existence of an HIV drug, 83.5% of the answers were correct for the transmission question, 94.3 % of the respondents correctly answered that it is sexual route and 86.1% were right in answering the parenteral route of transmission. The lowest success rate was for the highest prevalence in the world question, with only 18.3% of the correct answers; the low success rate was also found in the question about the difference between HIV and AIDS, with 18.5 % correctly answered, and at least one term (either HIV or AIDS) was correctly explained by 35.8 % of respondents. The success of respondents based on their answers is displayed in Table 2. According to the questionnaire, the highest knowledge of respondents was shown in the behavioural part of the study. In contrast, the poorest knowledge was displayed in answering the epidemiological questions. The highest amount of gathered points was 17 and the lowest one was 0. The average score was 7.3.
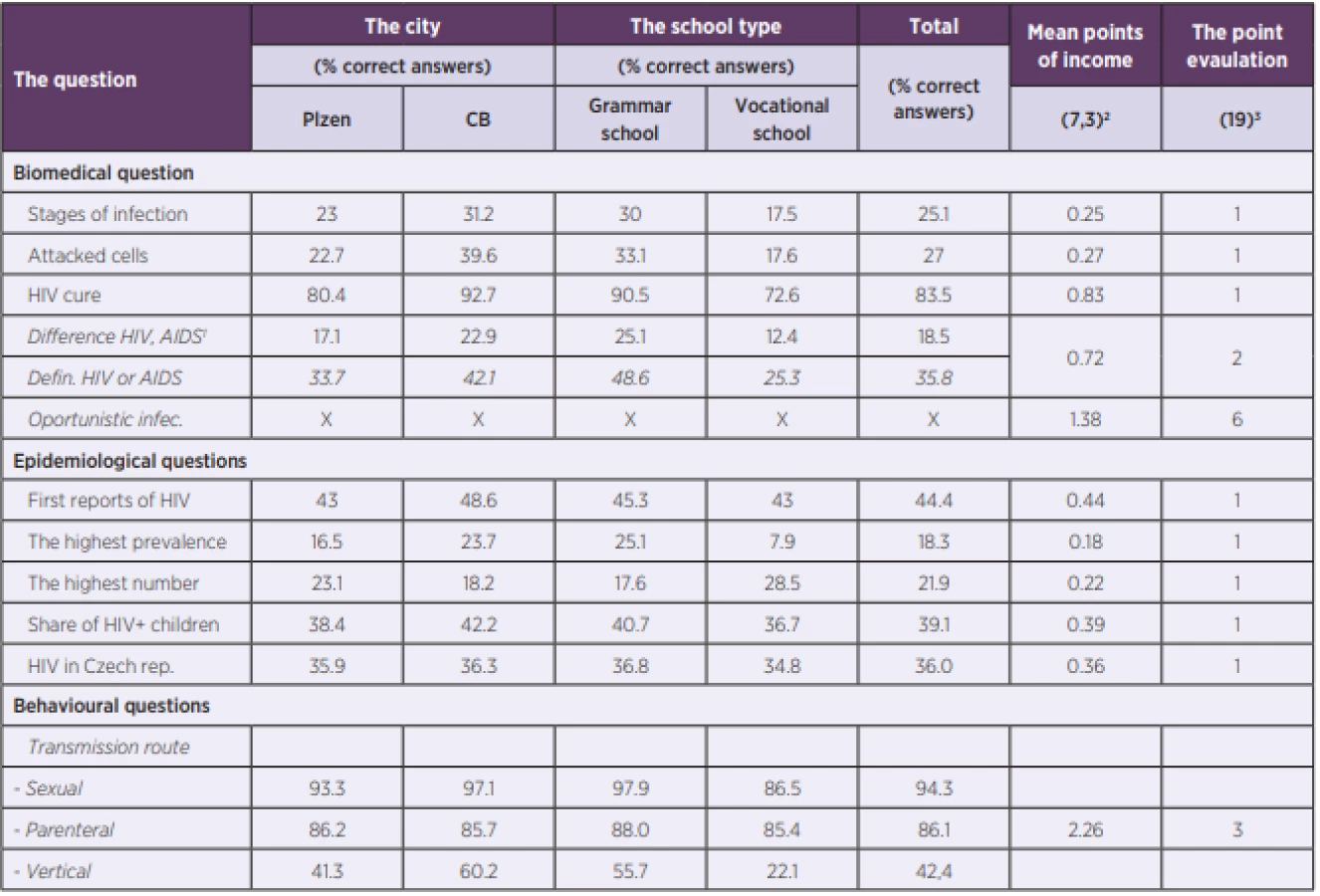
2The mean points of income for whole question.
3The maximum of the potencial points of income for each question.
The table displayes all questions from the questionnaire.
According to a previously defined level of health literacy, most of the respondents (67,3%) demonstrated acceptable knowledge. 27.5% had poor knowledge, which is approximately five times more than respondents who had very good knowledge (5.2%). Furthermore, 18-year--old respondents had the best knowledge, while the worst knowledge was shown by those aged 15 and 16. Women showed a higher level of knowledge than men. The highest difference in knowledge level was based on school type - students from grammar schools had higher knowledge than students from vocational schools. Table 3 shows the level of knowledge depending on the individual variables.
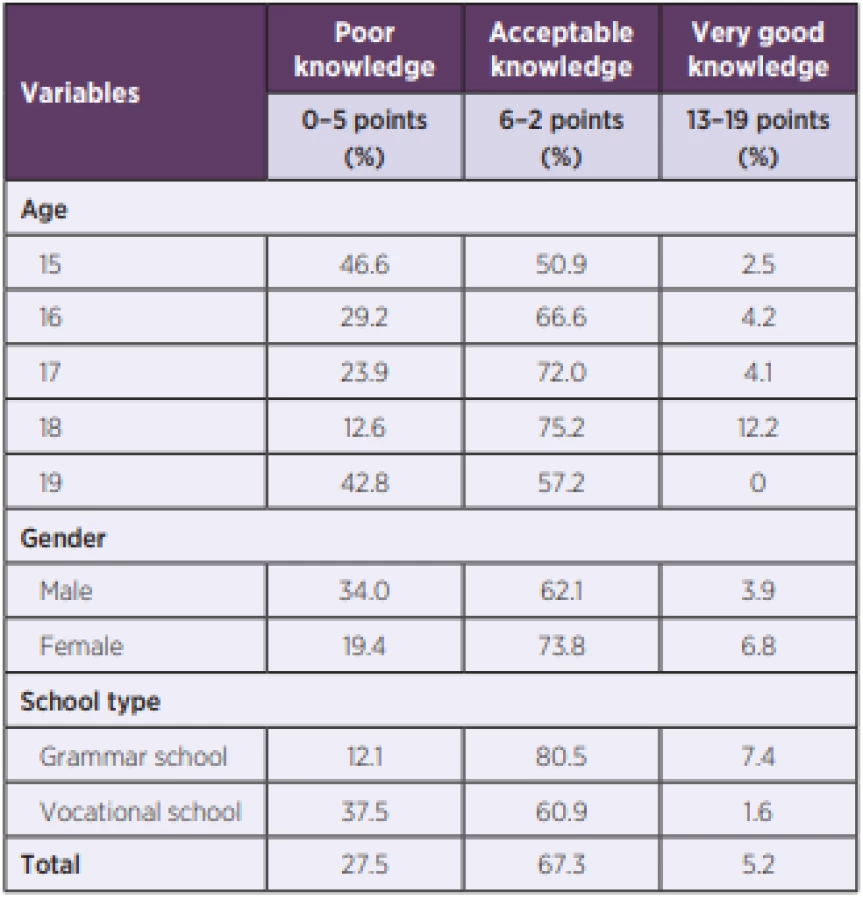
Table 4 demonstrates an association among each variable, the statistical significance of the influence of the variables, and the statistically significant difference in the averages of the variables. At a 5% significance level, a statistically significant difference was found between the average score and three variables: gender, city, and school type. At the same level of significance, a statistically significant effect of gender and type of school on the average score of points was shown. Using x2, an association between the level of knowledge and gender and the type of school was found at a 5% significance level.
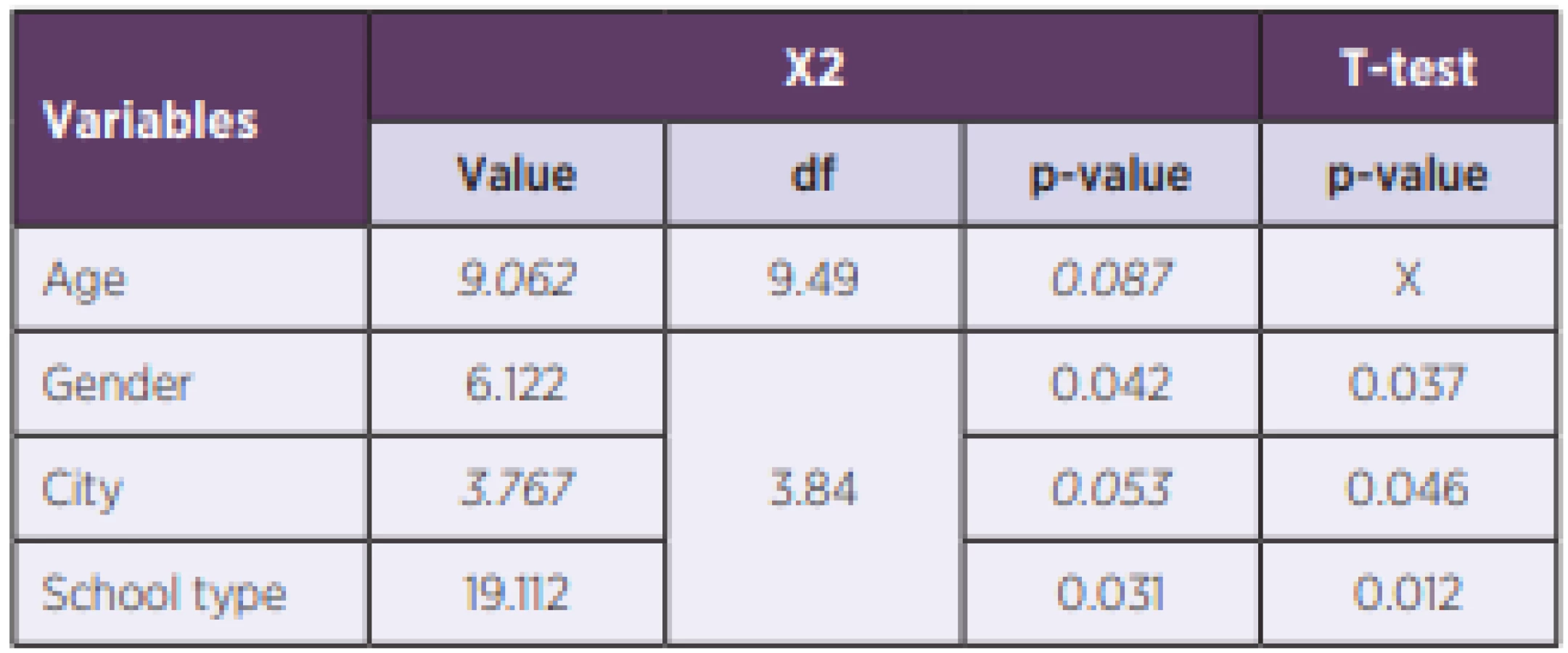
The research revealed a higher level of knowledge in women (x2 = 6,122), this difference was statistically significant (p = 0.042). It was also proved that grammar school students had better knowledge – the difference was statistically significant, too (p = 0.031). The statistically significant influence of age and place of study on knowledge level was not proved (age p = 0.087, city p = 0.053). The level of knowledge is therefore determined by gender (with better results in women) and the type of school (with better results at grammar schools). The internet (65.3%) and TV (53.1%) are the most common sources of information about HIV/AIDS. The respondents’ friends (36.5%) is the third most common source of information. Very few respondents rely on parents (12.0%) and school (9.7%) as a source of information. Specific to women, a gynaecologist (48.6% of women) was often reported as a source of information.
DISCUSSION
The implemented research was focused on the level of health knowledge among students of two types of schools – grammar schools and vocational schools in two different cites of the Czech Republic. In České Budějovice, the research was implemented only in grammar schools because there was no vocational school in the city that year. The research differed from other studies across numerous questions - it was focused on the actual knowledge of this topic and not just knowledge related to prevention (especially transmission, etc.). Because of this, it is not possible to compare the results with other studies. We could not find any research (similar to this one) focused on these two types of schools that were researched in the Czech Republic. The results show that most of the respondents have acceptable knowledge. Having said that, there is a significant difference between grammar school and vocational schools, and, similarly there are differences between women and men, however the type of school had a more important impact. The influence of the age was not statistically significant but the respondents of the higher-age-groups had better knowledge particularly in the comparison between 15 years old and 18 years old. However, there still is more than one-quarter of respondents that do not have sufficient health knowledge and therefore there is a higher risk of potential infection for this group.
One of the most important questions of this study is to know the difference between HIV and AIDS because this is an elemental attribute of terminology and prevention. Only 18.5 % of respondents of this study were able to explain the difference between these terms. 35.8% of respondents were able to explain at least one of these terms. The result was very different from the SZU study (2015) [24] where 70% of 1 627 respondents correctly answered the question ‘What is HIV?’ and 66.7% of them explained the term ‘AIDS’. Similar results were presented by another Czech study [20] where 67.6% of respondents knew that HIV is a virus. Even better results were presented by Otham (2015) [16] where 92.2% of 437 respondents in Iraq knew that HIV is a virus – the average age of respondents was 16.0 which is similar to our study (16.3). These differences can be explained by the fact that this was an open question in our study and it was a closed question in the study of Sajdová [20].
A majority of researches focused on HIV/AIDS knowledge are mostly interested in questions about HIV transmission. In our research, high knowledge of this issue was proved – 94.3% of respondents knew that HIV can be transmitted by sexual intercourse. Similar results were presented by Gupta (2013) [5] – 95.1% of the girls and 89.4% of the boys out of 215 respondents whose answer was also sexual intercourse. Similar values (94.3%) were presented in Othman’s study in Iraq (2015) [16]. Even higher values were found in other studies e. g.: SZU, 2015 (97.3%) [24], Sajdová, 2012 [20] and Weiss, 1998 (98%) [27]. In a study by Louda (2011) [9], it was presented that sexual intercourse as a way of transmission was the answer of all of the respondents. In spite of this, other studies show significantly lower values: 61.8% in India [8], approximately 50.0 % in Ethiopia [21]. The following routes of transmission were not so well known in our study, i.e. 86.1% reported parenteral transmission, and the results of the above studies remit about 90%. Only 42.4% reported vertical transmission, with women more likely to know this route. Sajdová’s research (2012) [20] reached a similar value (42.7%). Kumar (2012) [8] (65.7%) reported a higher share of knowledge of this transmission route. Studies by Bamise (2011) [2], Gupta (2011) [5] and Othman (2015) [16] achieved results in the range of 73.1–75.8%. Louda (2011) [9] reached the highest values of 81%. In our study, this question was open and therefore the wrong answers appeared with varying frequencies, with the most frequent wrong answer being saliva/kissing (37.4%). The SZU study (2015) [24] found similar results (32.9%) in another Czech study (Weiss, Rabušič, Louda) [27], [17], [9] showing lower values, around 20%. Compared to foreign studies, our values were low, e.g. in Bamise’s study (2011) [2] it was 53,7%, in Othman’s (2015) [16] it was 56,8 %. Another common answer was transmission via biting insects (21.8%). This result is lower than in the study of SZU (2015) [24] but it corresponds to the studies of Louda (2011) [9], Weiss (1998) [27] and Gao (2012) [4]. Just as Alhasawi (2019) [1] found some absurd results in his study (58,4% said that transmission can be caused by sharing a comb), our study also showed some absurd responses such as drinking milk, eating faeces, etc.
Our study proved that respondents correctly answered the question of curing HIV infection – only 16.5% answered that HIV infection can be cured. Similar results were presented by Rabušič (2003) [17] – 15% and for example Gao (2012) [4] – 15.3%. Higher values were found in other studies e.g. 50% of respondents in Ethiopia [21] and 78.3% of respondents in Iraq [16] answered that HIV can be cured. These numbers could be explained by mass media that often present findings of HIV cure and that the infection is not lethal anymore. The influence of mass media most probably plays a role in this.
While the SZU survey (2015) [24] has not shown a gender-related dependence of HIV knowledge, our research has demonstrated and verified this dependence in favour of women, which is consistent with the Swenson (2010) [23] study from the USA. However, other researches do not show differences in knowledge, e.g. Gupta (2011) [5] or Shiferaw (2011) [21]. On the other hand, the opposite results (men have higher knowledge than women) were found in the research of Alhasawi (2019) [1] and Oljira (2013) [15] in Kuwait and Ethiopia. The association between knowledge of HIV/AIDS and gender seems to be culturally determined, since we can observe higher knowledge among men in Islamic countries, while in other countries (where Islam is not a religion practised by a majority, e.g. India) the difference is not demonstrable. Conversely, in developed countries (e.g the USA), knowledge is higher among women. However, this is also speculative, as Tapia-Aguirre, 2004 [25], for example, showed that in adolescents in Mexico, women have statistically significantly higher knowledge.
Studies that we compare with our study, including SZU, 2015 [24] found an association between age (attended grade) and level of knowledge. In these studies, there is a correlation between older age and higher knowledge. This association has not proved to be significant in our research.
An important question of our research, which did not measure knowledge, was where respondents search for information. According to our study, respondents search the information on the internet (65.3%) and on TV (53.1%). On the other hand, school as a source of information was mentioned only by 12% of the respondents. These results are significantly different from SZU (2015) [24] where school was the main source of information for 50,8% and the Internet for only 33,3% of the respondents. There might be a correlation between the source of information and the economic level of the country. In developing countries like Nigeria [2], India [5], [8], Iraq [16], Ethiopia [21] or China [4], the main source of information was TV or radio. This fact can also be caused by the year of publication – massive internet usage is usually connected to second decade of 21st century.
In 2012, Sajdová [20] implemented a study comparing the knowledge of high school and grammar school students and found the same results as we did – grammar school students have a higher level of knowledge. Statistically significant differences are also pointed out by Bamise (2011) [2] in Nigeria and Alhasawi (2019) [1] in Kuwait, where science students had a higher level of knowledge than art students. Based on this association, it is possible to consider the type of school as a protective or risk factor.
Our study proved that 67,3% of respondents have good (acceptable) knowledge. Rabušic (2003) [17] also claims that adolescents in the Czech Republic have good know-ledge. Research in New York [22] as well as another research in the USA [19] point to a high level of knowledge among respondents, but mainly in some areas, especially prevention, testing and transmission routes, which is consistent with our results.
Despite a quite high number of respondents, we know the study implemented only in two cities is limiting for generalization of results. However, next comparative studies with a higher number of the respondents and particularly with a higher number of included cities could be processed. Also the unequal distribution of the types of the schools in the cities (absence of vocational schools in České Budějovice) brings certain limitations of the study especially in the comparison between these cities.
Finally, we would like to thank the headmasters and teachers of the schools integrated in this study and of course all of the participants who were included in this research.
CONCLUSION
Our study showed that most respondents have acceptable health knowledge of HIV infection, yet their knowledge is very unbalanced. Respondents demonstrated acceptable knowledge in questions related to prevention and transmission. However, regarding the explanation of the difference between HIV and AIDS, their knowledge is significantly lower. The study discovered a very low level of knowledge related to HIV expansion in the world whereas at least basic knowledge about the distribution of this infection is a part of primary prevention. Adolescents did not demonstrate sufficient knowledge in these questions. However, respondents with higher knowledge (typically, grammar schools’ students and women) did not prove sufficient knowledge only in some of them.
The results suggest that prevention is targeted, which seems to focus sufficiently on the ways of infection transmission, and other peculiarities of this widespread issue that contribute to reducing exposure to infection are lagging behind.
This study shows the unequal knowledge of students in two different types of schools and in the individual area. Based on this, we recommend unifying the quantity of information for both types of schools because less information can raise the risk of exposition to the infection. Then, the information should be distributed in a more balanced way in every area of knowledge – not only as a biomedical topic, but also as a social and behavioural issue. Also, the students should show they are able to use this information, particularly in their everyday lives.
Do redakce došlo dne 31. 1. 2020.
Adresa pro korespondenci:
RNDr. Jiří Preis, Ph.D.
Katedra geografie, Fakulta ekonomická ZČU
Univerzitní 22
301 00 Plzeň
e-mail: jpreis@kge.zcu.cz
Sources
1. Alhasawi A, Grover SB, Sadek A, Ashoor I, Alkhabbaz I, Almasri S. Assessing HIV/AIDS Knowledge, Awareness, and Attitudes among Senior High School Students in Kuwait. Medical principles and practice. International journal of the Kuwait University, Health Science Centre, 2019;28(5):470–476.
2. Bamise OF, Bamise CT, Adedigba MA. Knowledge of HIV/AIDS among secondary school adolescents in Osun state, Nigeria. Nigerian journal of clinical practice, 2011;14(3):338–344.
3. Country Progres Report, The Czech Republic, Global AIDS Responde Progress Report 2015. Prague, 2016
4. Gao X, Wu Y, Zhang Y, Zhang N, Tang J, Qiu J, Lin X, Du Y. Effectiveness of School-based Education on HIV/AIDS Knowledge, Attitude, and Behavior among Secondary School Students in Wuhan, China. PLoS ONE, 2012;7(9):e44881.
5. Gupta P, Anjum F, Bhardwaj P, Srivastav J, Zaidi ZH. Knowledge About HIV/AIDS Among Secondary School Students. North American journal of medical sciences, 2013;5(2): 119–123.
6. He L, Jin Y, Ren X, Wang L, Nie Z, Gu Q, Yao Y. Sexual Activity and HIV-Related Knowledge among Secondary School Students in China. The Eurasian journal of medicine, 2019;51(1):49–52.
7. Kirby Douglas B, Laris BA, Rolleri Lori A. Sex and HIV education programs: their impact on sexual behaviours of young people throughout the world. Journal of adolescent Health, 2007;40(3):206–217.
8. Kumar P, Pore P, Patil U. HIV/AIDS-related KAP among high-school students of municipal corporation school in Pune. An interventional study. Natl J Community Med, 2012; 3(1):74–79.
9. Louda P. Komparativní analýza úrovně znalostí v oblasti lidské sexuality mezi studenty středních škol a gymnázií. Bachelor’s thesis, 2011. Charles University.
10. Mičulková V. Prevence infekce HIV. PhD dissertation [online]. Brno, Masaryk University, 2018 [cit. 2019-6-8]. Dostupné na www:
https://is.muni.cz/th/xh4df/Disertacni_prace.pdf.
11. MŠMT, Rámcový vzdělávací program pro gymnázia. Výzkumný ústav pedagogický v Praze. Praha, 2007. ISBN 978-80-87000-11-3.
12. MŠMT, Rámcový vzdělávací program pro střední odborné vzdělávání. Národní ústav odborného vzdělávání. Praha, 2009.
13. MŠMT, Rámcový vzdělávací program pro základní vzdělávání. Národní ústav pro vzdělávání. Praha, 2017.
14. Odeigah L, Rasaki SO, Ajibola AF, Hafsat AA, Sule AG, Musah, Y. High risk sexual behavior among adolescent senior secondary school students in Nigeria. African health sciences, 2019;19(1):1467–1477.
15. Oljira L, Berhane Y, Worku A. Assessment of comprehensive HIV/AIDS knowledge level among in-school adolescents in eastern Ethiopia. Journal of the International AIDS Society, 2013;16(1):17349.
16. Othman SM. Knowledge about HIV/AIDS among high school students in Erbil city/Iraq. Global journal of health science, 2015;7(1):16.
17. Rabusic L, Kepáková K. Adolescent sexual behavior and the HIV/AIDS risk in the Czech Republic. Revija za sociologiju, 2003;34(3–4):189.
18. Roční zprávy o výskytu a šíření HIV/AIDS v ČR, Státní zdravotní ústav, online. 2019-5-28. Dostupné na www: http://www.szu.cz/tema/prevence/rocni-zpravy-o-vyskytu-a-sireni-hiv-aids-v-cr?highlightWords=hiv.
19. Rotheram-Borus MJ, Gillis JR, Reid HM, Fernandez MI, Gwadz M. HIV testing, behaviors, and knowledge among adolescents at high risk. Journal of Adolescent Health, 1997;20(3):216–225.
20. Sajdlová M. Znalosti a postoje k problematice HIV/AIDS u dospívajících ve vybraném regionu. Diploma thesis, 2012. Charles Univesity.
21. Shiferaw Y, Alemu A, Girma A, Getahun A, Kassa A, Gashaw A, Gelaw B. Assessment of knowledge, attitude and risk behaviors towards HIV/AIDS and other sexual transmitted infection among preparatory students of Gondar town, north west Ethiopia. BMC research notes, 2011;4(1):505.
22. Sikand A, Fisher M, Friedman, SB. AIDS knowledge, concerns, and behavioral changes among inner-city high school students. Journal of adolescent health, 1996;18(5):325–328.
23. Swenson RR, Rizzo CJ, Brown LK, Vanable PA, Carey MP, Valois RF, Romer D. HIV knowledge and its contribution to sexual health behaviors of low-income African American adolescents. Journal of the National Medical Association, 2010;102(12):1173–1182.
24. Šikolová V, Fialová A. Výsledky dotazníkového šetření k výuce problematiky HIV/AIDS na základních školách a víceletých gymnáziích. Státní zdravotní ústav, 2015.
25. Tapia-Aguirre V, Arillo-Santillán E, Allen B, Angeles-Llerenas A, Cruz-Valdéz A, Lazcano-Ponce E. Associations among condom use, sexual behavior, and knowledge about HIV/AIDS. A study of 13,293 public school students. Archives of Medical Research, 2004;35(4):334–343.
26. Thanavanh B, Harun-Or-Rashid M, Kasuya H, Sakamoto J. Knowledge, attitudes and practices regarding HIV/AIDS among male high school students in Lao People’s Democratic Republic. Journal of the International AIDS society, 2013;16(1):17387.
27. Kucera Z, Weiss P, Sverakova M. Risk Factors in the Sexual Behaviour of Czech Adolescents. International journal of adolescent medicine and health, 1998;10(2):129–140.
Labels
Hygiene and epidemiology Medical virology Clinical microbiologyArticle was published in
Epidemiology, Microbiology, Immunology

2020 Issue 4
Most read in this issue
- Data from the first wave of Covid-19 from the Central Military Hospital, Prague, Czech Republic
- Severe community-acquired pneumonia in intensive care
- Individualized dosing of vancomycin in geriatric patients
- MAIT cells, their biological and medical significance