
Forensic toxicological implications of pleural effusion; an autopsy case of drug overdose
Forenzně toxikologické dopady pleurálního výpotku; autoptický případ předávkování drogami
Prezentujeme případ smrtelné otravy psychotropními drogami. Kvantitativní toxikologická analýza prokázala ve femorální krvi tyto koncentrace fenobarbitalu, promethazinu, chlorpromazinu, alprazolamu a bromazepamu: 69.51μg/ml, 32.73μg/ml 24.76μg/ml, 0.04μg/ml and 0.31μg/ml; velké množství těchto látek bylo prokázáno i v žaludečním obsahu. Soudíme, že příčinou smrti bylo především předávkování fenobarbitalem, promethazinem a chlorpromazinem při jejich masivní ingesci. Dále diskutujeme přínos pleurálního výpotku jako alternativního vzorku pro toxikologické vyšetření.
Keywords:
mnohočetné drogy – otrava – kapalinová chromatografie s hmotnostní spektrometrií – fenobarbital – pleurální výpotek
Authors:
Naoko Tanaka 1; Hiroshi Kinoshita 1; Azumi Kuse 2; Mayo Takatsu 3; Mostofa Jamal 1; Mitsuru Kumihashi 1; Yasushi Nagasaki 3; Migiwa Asano 2; Yasuhiro Ueno 2; Kiyoshi Ameno 1
Authors‘ workplace:
Department of Forensic Medicine, Faculty of Medicine, Kagawa University
1; Division of Legal Medicine, Department of Environmental Health and Safety, Kobe University Graduate School
of Medicine, 7-5-1, Kusunoki-cho, Chuo-ku, Kobe, 650-0017, Japan
2; Hyogo Medical Examiners Office, Arata-cho 2-1-31, Hyogo-ku, Kobe, 652-0032, Japan
3; -1, Miki, Kita, Kagawa, 761-079 , Japan
1750
Published in:
Soud Lék., 57, 2012, No. 3, p. 48-50
Category:
Original Article
Overview
A fatal poisoning case involving multiple psychotropic drugs is presented. Quantitative toxicological analysis showed that the concentrations of phenobarbital, promethazine, chlorpromazine, alprazolam and bromazepam in the femoral blood were 69.51μg/ml, 32.73μg/ml 24.76μg/ml, 0.04μg/ml and 0.31μg/ml respectively, and large amounts of drugs were also detected in the stomach contents. We concluded that the cause of death was mainly due to overdose of phenobarbital, promethazine and chlorpromazine by massive ingestion, and we also discuss the value of pleural effusions as an alternative specimen for toxicological examination.
Keywords:
multiple drug – poisoning – liquid chromatography mass spectrometry – phenobarbital – pleural effusion
Toxicity in poisoning cases is usually evaluated from concentrations of the drugs in the blood, based on previous reports of fatal or non-fatal cases (17). Pleural effusions are occasionally collected in forensic practice as alternative specimens in toxicological examination, in cases where clean blood samples are not available (6). Here we report a case of death due to the toxicity of multiple psychotropic drugs, and we discuss the usefulness of pleural effusions as alternative specimens in toxicological examination.
CASE REPORT
A female in her twenties was found dead in her room. The subsequent police investigation revealed that the deceased had been receiving therapy for mental disorder and had been receiving prescribed drugs.
The deceased was 165 cm in height and 45 kg in weight. External examination revealed slight abrasion on her left lower leg. The heart weighed 173g, containing 30ml of blood without coagulum. The brain weighed 1380g and was slightly edematous. The left and right lungs weighed 485g and 504g, respectively, and were moderately congested. The stomach contained approximately 400 ml of brownish fluid with granules. There were no notable changes, other than congestion. Drug screening test using a TriageTM (Biosite Diagnostic Inc, San Diego, USA) panel was positive for barbiturates. Postmortem samples such as femoral venous blood, urine, bilateral pleural effusions and the stomach contents were collected for toxicological examination.
Toxicological analysis was performed using a liquid chromatography-mass spectrometry (Quattro micro® API mass spectrometer in combination with 2695 alliance system®, Waters, Milford, MA, USA). Its operation and the preparation of the samples were in accordance with the manufacturer’s specifications (16). Quantitation of ethanol was performed using a head-space gas-chromatography.
RESULTS AND DISCUSSION
Toxicological analysis identified the presence of phenobarbital, promethazine, chlorpromazine, alprazolam and bromazepam. However, no ethanol was detected in the blood or urine. Table 1 shows the quantitation of each drug in the victim’s blood, urine, left/right pleural effusion and stomach contents, and also summarizes their fatal and therapeutic levels (13,14,15,17). The victim’s femoral blood concentrations of phenobarbital, promethazine, chlorpromazine, alprazolam and bromazepam were 69.51μg/ml, 32.73μg/ml 24.76μg/ml, 0.04μg/ml and 0.31μg/ml, respectively. The concentration of phenobarbital, promethazine and chlorpromazine exceeded fatal levels (15,17), and the victim died during the absorption phase of these drugs, as large amount of these drugs were detected in the stomach. The concentration of alprazolam and bromazepam are around the therapeutic levels (13,17), and were found in the elimination phase, as the concentration of each drug in stomach contents is similar to these in blood. From the autopsy findings and the results of the toxicological examination, we concluded that death was mainly due to the combined toxicity of phenobarbital, promethazine and chlorpromazine by massive ingestion, while alprazolam and bromazepam may also have made a small contribution to her death.
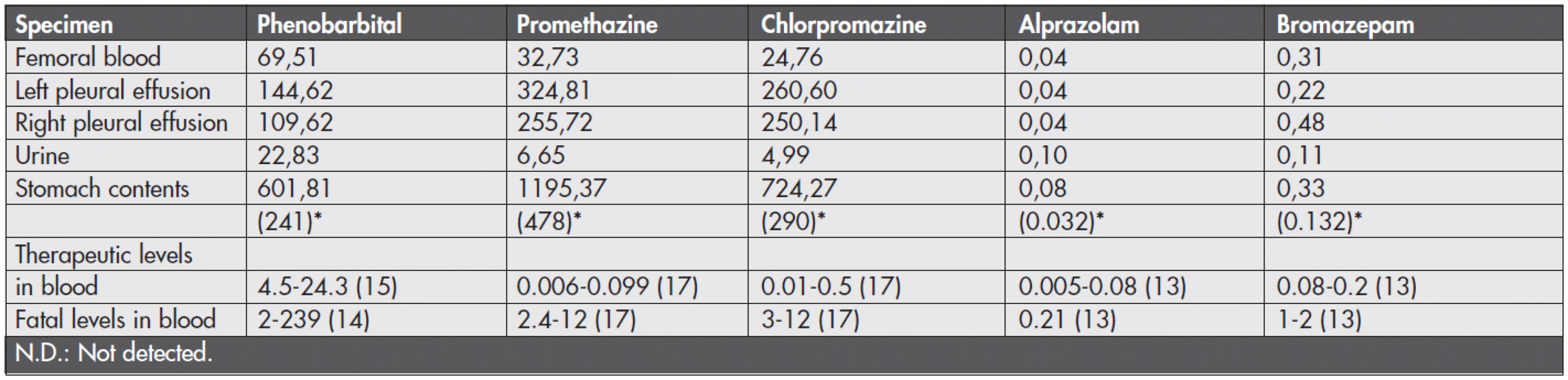
As shown in Table 1, the concentrations of promethazine and chlorpromazine in the pleural effusion were over 7.8 and about 10 times higher than those in the femoral blood, while the concentration of phenobarbital in the samples of the pleural effusion were about 1.5-2 times higher than in the femoral blood. These phenomena may have been due to the postmortem redistribution of the drugs from lung or liver, and postmortem diffusion of drugs from the stomach (3,5,9,11,12). On the other hand, the concentrations of alprazolam and bromazepam in pleural effusions were similar to those found in the femoral blood.
We should to pay attention to the pharmacokinetic properties of each drug. Drugs which have large distribution volume (Vd) value, are also distributed in surrounding tissue (1). The Vd values of drugs detected in the present case were as follows; phenobarbital (0.5L/kg), promethazine (13L/kg), chlorpromazine (21L/kg), alprazolam (0.7L/kg), bromazepam (0.9L/kg) (8). Pleural effusions are formed by exudation from the edematous and congestive lungs. Both promethazine and chlorpromazine are basic drugs with large Vd values, and the concentration of promethazine and chlorpromazine in the lungs were higher than in the blood, respectively (4,7). Diffusion of promethazine and chlorpromazine from the lungs to the pleural effusions may be observed during the postmortem period, as reported previously (9,10). On the other hand, as the Vd values of phenobarbital, alprazolam and bromazepam were relatively small, their concentrations in the pleural effusion may not have been highly increment. The apparent Vd of more than 3-4L/kg is a good predictor that a drug is liable to cause postmortem redistribution (2). These pharmacokinetic properties of each drug may cause significant postmortem redistribution to pleural effusions.
The concentration of phenobarbital, promethazine and chlorpromazine in the pleural effusion in the left thoracic cavity were higher than those in the right thoracic cavity. Since higher concentration of these drugs were detected in the stomach contents, and in consideration of the anatomical structure and relationship of the organs, postmortem diffusion from the stomach should also be considered (12).
The present case indicates that we have to consider the postmortem diffusion or redistribution of drugs when evaluating postmortem data. Since the pleural effusion is easily collected at the time of autopsy or inspection, and contains relatively high concentration of drugs, it would be a good predictor for the toxicological screening. As like alprazolam and bromazepam in this case, drugs with low Vd value and death during elimination phase, the drug concentrations in the pleural effusion may be applicable to estimate the blood levels at the time of death. However, it may not be suitable for quantitative analysis, especially in some basic drugs. Concentration of the pleural effusion is rarely related to the ranges of blood concentration (6). In the present case, concentration of phenobarbital, promethazine and chlorpromazine, in pleural effusion are inapplicable to the estimation of the concentration in femoral blood. The role of pharmacokinetic properties of drugs may be an interesting target for the study of postmortem redistribution. The usefulness of the pleural effusion in toxicological examination is not clear and additional studies and case report will be required.
Address for correspondence:
Dr. H. Kinoshita,
Department of Forensic Medicine, Faculty of Medicine,
Kagawa University
1750-1, Miki, Kita, Kagawa, 761-0793, Japan
tel: +81-87-891-2140 fax: +81-87-891-2141
e-mail: kinochin@med.kagawa-u.ac.jp
Sources
1. Ellenhorn MJ, Barceloux DG. Medical Toxicology, diagnosis and treatment of human poisoning. New York: Elsevier; 1988, pp 104-130.
2. Hilberg T, Ripel Ā, Slørdal L, Bjørneboe A, MŅrland J. The extent of postmortem drug redistribution in a rat model. J Forensic Sci 1999; 44 : 956-962.
3. Jones GR, Pounder DJ. Site dependence of drug concentrations in postmortem blood – a case study. J Anal Toxicol 1987; 11 : 186-190.
4. Kageura M, Hara K, Hieda Y, Takamoto M, Fukuma Y, Kashimura S. Forensic toxicological findings in a death from combined drug comprised of Phenobarbital, promethazine and chlorpromazine. Res Pract Fortens Med 1987; 30 : 83-87.
5. Kinoshita H, Nishiguchi M, Kasuda S, et al. Forensic toxicological implication of an autopsy case of mixed drug overdose involving clomipramine, chlorpromazine and flunitrazepam. Soud Lek. 2008; 53 : 28-30.
6. Knight B. Forensic Pathology (2nd ed). London: Arnold; 1996, pp.531-541.
7. Koreeda A, Yonemitsu K, Ng’walali PM, Muraoka N, Tsunenari S. Clocapramine -related fatality postmortem drug levels in multiple psychoactive drug poisoning. Forensic Sci Int 2001; 122 : 48-51.
8. Moffat AC, Osselton MD, Widdop B, editors. Clark’s analysis of drug and poisons, 3rd edition. London, Chicago: Pharmaceutical Press; 2004.
9. Moriya F, Hashimoto Y. Redistribution of basic drugs into cardiac blood from surrounding tissues during early-stages postmortem. J Forensic Sci 1999; 44 : 10-16.
10. Moriya F. Pitfalls and cautions in analysis of drug and poisons. In: Suzuki O and Watanabe K. eds. Drugs and poisons in humans. A handbook of practical analysis. Berlin Heidelberg: Springer-Verlag; 2005, pp17-24.
11. Pounder DJ, Jones GR. Post-mortem drug redistribution – a toxicological nightmare. Forensic Sci Int 1990; 45 : 253-263.
12. Pounder DJ, Fuke C, Cox DE, Smith D, Kuroda N. Postmortem diffusion of drugs from gastric residue an experimental study. Am J Forensic Med Pathol 1996; 17 : 1-7.
13. Schulz M, Schmoldt A. Therapeutic and toxic blood concentrations of more than 800 drugs and other xenobiotics. Pharmazie 2003; 58 : 447-474.
14. Stead AH, Moffat AC. Interpretation of therapeutic, toxic and fatal phenobarbitone blood concentrations by the use of concentration-response and toxicity probability curves. J Forens Sci Soc 1982; 22 : 47-56.
15. Stead AH, Hook W, Moffat AC, Berry D. Therapeutic, toxic and fatal blood concentration ranges of antiepileptic drugs as an aid to the interpretation of analytical data. Hum Toxicol 1983; 2 : 135-147.
16. Tanaka N, Kinoshita H, Takatsu M, et al. A fatal case of butane gas inhalation. Current Studies of Environmental and Medical Sciences 2010; 3 : 15-16.
17. Winek CL, Wahba WW, Winek CL Jr, Balzer TW. Drug and chemical blood-level data 2001. Forensic Sci Int 2001; 122 : 107-123.
Labels
Anatomical pathology Forensic medical examiner ToxicologyArticle was published in
Forensic Medicine

2012 Issue 3
Most read in this issue
- Primary and secondary complex suicide. A 30-year retrospective suicide
- Suddenly deceased young individuals autopsied at the Department of forensic medicine, Brno – analysis
- Forensic toxicological implications of pleural effusion; an autopsy case of drug overdose
- The year 1989 and its reflection in the forensic medicine