
Electrical burns in adults
Authors:
S. Al-Benna
Authors‘ workplace:
Division of Plastic Surgery, Sheikh Khalifa Medical City, Abu Dhabi, United Arab Emirates
Published in:
ACTA CHIRURGIAE PLASTICAE, 65, 2, 2023, pp. 66-69
doi:
https://doi.org/10.48095/ccachp202366
Introduction
Electrical burns account for up to 10% of burns admissions worldwide and have a potentially devastating capacity for functional and aesthetic sequelae [1]. The pathophysiology of an electrical burn depends on the voltage, current flow, and tissue resistance [1]. Electrical burns can result from low-voltage (< 1,000W) or high-voltage (>1,000W) currents [1–6] (Fig. 1). Depending on the mechanism of injury, the victim may suffer from a flash or arc burn, this is usually a superficial burn or a contact burn where electric current passes through the body [1]. The damage caused by electrical burns occurs by two active mechanisms, thermal action at the body level (joule heating) and electrolytic action at the cell level when the current passes through the tissue (cell lysis by electroporation) [1]. The heating causes coagulative necrosis of the cells [1]. The impact from the latter mechanism bears greater consequences – cell membrane disruption leading to tissue loss and death [1].

Major complications arise when progressive devitalisation of tissues secondary to thrombosis of affected blood vessels [1]. This leads to deep tissue damage and may result in subsequent loss of organs or limbs [7–14]. Higher tissue water content improves conduction and worsens resultant damage [1]. Local oedema around damaged tissue causes progressive compression and obliteration of the microcirculation that leads to compartment syndrome [1–4]. Other complications include neurological sequelae, cardiac arrhythmias and renal failure [1–14].
Over the last three decades, regulation in electrical safety has improved considerably, and it is widely believed that public policy and education has changed the epidemiology of electrical burn injuries [2–4,6,7,9,11,13,14]. Current prevention strategies include both active measures (education) and passive measures (product design, environmental change, legislation, and regulation) [15–24]. These have included changes such as redesign of electrical plugs, burying power lines, making high-voltage sources less accessible, and undertaking educational messages to school children about risk taking; and parents about preventing access to electricity (such as covering electrical outlets) [5,25,26].
Concerning the mechanism of potentially catastrophic injury, there exist limited Middle Eastern data [15–17]. The aim of this study was to describe the epidemiology, presentation, management and complications of electrical burn injuries in adults admitted to a tertiary burns centre in the Middle East.
Material and methods
A retrospective case note review of all adults with electrical burns admitted to the tertiary burns centre of Sheikh Khalifa Medical City, Abu Dhabi were analysed. The study received approval from the local human research ethics committee (Ethics Approval Reference Number: REC-14.10.2015 [RS-396]). Procedures used in this study are in line with the ethical principles of the Helsinki Declaration. Data are presented as means ± standard errors of the means [16]. The following variables were considered: age, sex, voltage, mechanism of injury, total body surface area (TBSA) and length of hospital stay. Patients who arrived dead after electrical burn or those admitted to the general wards were excluded. On arrival, the patients underwent immediate cardiopulmonary resuscitation and investigation for other associated injuries. Intravenous fluid resuscitation, when required, was made using compound Ringer’s lactate solution. Patients were commenced on ranitidine and intravenous opioids. Antibiotics were not used unless there was evidence of systemic or localized infection. Patients were monitored closely for vital signs and urine output. Daily blood investigations for packed cell volume and electrolyte disturbances were performed. Urinalysis was carried out to rule out myoglobinuria, which, if found, was treated with mannitol and sodium bicarbonate. Minor injuries were managed conservatively with Aquacel Ag dressings. Fasciotomy was performed if compartment syndrome was suspected [27]. Full thickness burns were treated with early debridement. Wound re-surfacing was achieved by split thickness skin grafting, or by local or pedicled flap coverage. All patients had subsequent wound and rehabilitation follow-up after discharge.
Results
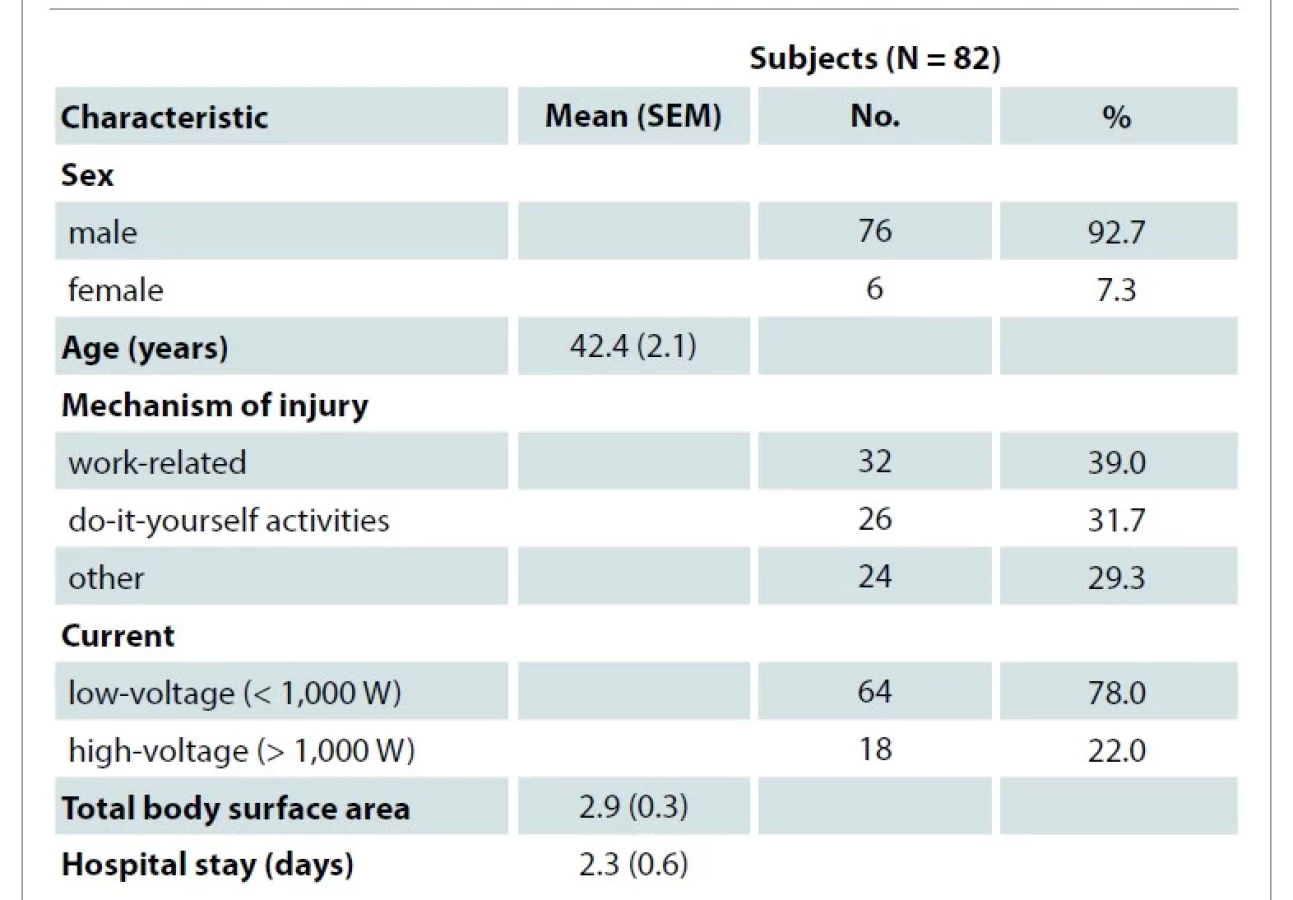
Eighty-two patients were admitted to a tertiary burns centre with electrical burns (Tab. 1). The mean age of patients was 40 ± 2 years. Seventy-six patients (93%) were males. The most common activities associated with injury were manual work and do-it-yourself (DIY) activities. A low voltage (< 1,000 W) power source was involved in 64 (78%) cases. Mean TBSA involved was 3 ± 1%. All cases involved injury to the upper limbs. The mean hospital stay was 2 ± 1 days (Tab. 1).
Patients presented with injuries varying from small, partial thickness burns to larger, full thickness burns. Given the absence of a standard injury classification system, they were categorised on the basis of burn depth and exposure/injury to critical structures: 53% suffered burns treated conservatively, 19% patients suffered deep partial thickness or full thickness burns treated by excision and split skin grafting, 7% required surgical decompression in addition to excision and split skin grafting, and 21% required wound coverage with local or pedicled flaps after burn excision (Tab. 2).
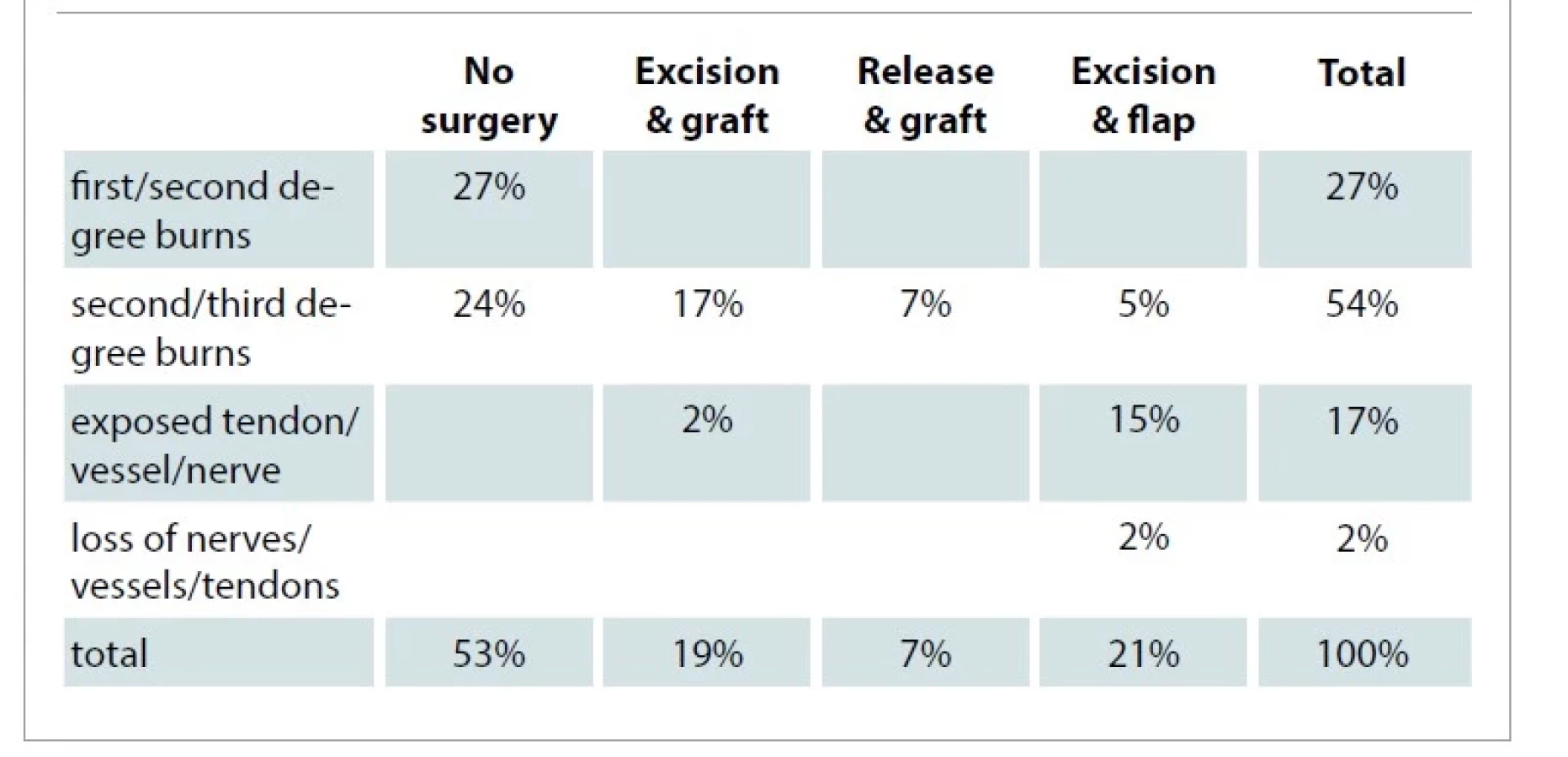
Surgery was dependent on the degree of the injury. Out of these 82 patients, 44 (53%) required no surgery, 16 (19%) underwent primary excision and grafting, 6 (7%) required release and grafting, 4 (5%) required local tissue rearrangement and 18 (21%) required flap coverage (Tab. 2).
Discussion
In this study, a low voltage source was involved in 78% of cases and resulted in flash burns which were successfully managed non-operatively. In more severe cases, fasciotomy was performed due to suspected compartment syndrome [27]. Manual work and household DIY activities accounted for almost three quarters of adult electrical injuries. It is possible that poor training and education may have contributed to these injuries, highlighting their preventable nature [26,27].
Previous reports from industrialised nations in the 1970s showed relatively high rates of high-voltage electrical injuries, with major tissue destruction and burns, ranging up to 80% TBSA at major trauma centres [26–31]. The data in this series is in keeping with previous observations of an apparent decline in rates of devastating high-voltage injuries in very high human development countries [1,3,5,7,9,12,26,32]. Furthermore, the severity of burn injuries has decreased, likely due to less exposure to high-voltage electrical sources [2–4,26]. This has resulted in a relatively higher proportion of low-voltage, low mortality injuries. This change in presentation and referral patterns may be due to improved safety measures and legislation within the United Arab Emirates [13]. This study demonstrates the severity of electrical burns and its serious consequences. Poverty and lack of effective safety policies and measures allows high-voltage sources to remain a significant danger in low - and middle-income countries [33,34].
Conclusion
Electrical burns make up a small percentage of admissions to most burn units [1–14]. However, these injuries are challenging to treat and have the potential to cause significant morbidity and mortality [1–4]. The sequelae of electrical burns are both functionally and cosmetically debilitating [1,10]. Their management may be further complicated by systemic effects of electrical injury [1–4,6–8]. Additionally, the assessment of the extent and depth of the damage may be inaccurate due to the propagation of current and, hence, the injuries along deep tissue planes result in those that are much more severe than external appearances would suggest [1,7,11].
Acknowledgements: None
Disclosure statement: The author has no conflicts of interest to disclose. The author declares that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the local human research ethics committee; Ethics Approval Reference Number: REC-14.10.2015 [RS-396] and with the Helsinki declaration and its later amendments or comparable ethical standards.
Role of author: Sammy Al-Benna – concept, design, resources, materials, data collection and/or processing, analysis and/or interpretation, writing manuscript, critical review.
Sammy Al-Benna, M.B. Ch.B., Ph.D., FA.P.Ä.C.
Division of Plastic and Reconstructive Surgery
Faculty of Medicine and Health Sciences
Stellenbosch University and Tygerberg
Academic Hospital
Francie van Zijl Drive,
PO Box 241
Cape Town 8000
South Africa
e-mail: sammyalbenna@doctors.org.uk
Submitted: 15. 7. 2022
Accepted: 17. 6. 2023
Sources
1. Neligan PC., Song D. Plastic surgery: volume 4: trunk and lower extremity. New York (USA): Elsevier Inc. 2013 : 393–434.
2. Lengyel P., Frišman E., Babík J., et al. Electrical burns in our workplace. Acta Chir Plast. 2014, 56(1–2): 13–14.
3. Sedova SV. Surgery for hand deformities due to electrical injury. Acta Chir Plast. 1989, 31(4): 201–208.
4. Lipový B., Rihová H., Kaloudová Y., et al. The importance of a multidisciplinary approach in the treatment of mutilating electrical injury: a case study. Acta Chir Plast. 2010, 52(2–4): 61–64.
5. Baker PA., Al-Benna S., Thompson R., et al. The “red gold” rush and severe electrical burns. Burns. 2008, 34(6): 885–887.
6. Kaloudová Y., Sín R., Rihová H., et al. High voltage electrical injuries. Acta Chir Plast. 2006, 48(4): 119–122.
7. Crkvenjas Z., Tymonová J., Adámková M., et al. Surgical treatment of electrical burns by local flap plastic surgery. Acta Chir Plast. 2005, 47(1): 10–12.
8. Mohammadi AA., Amini M., Mehrabani D., et al. A survey on 30 months electrical burns in Shiraz University of Medical Sciences Burn Hospital. Burns. 2008, 34(1): 111–113.
9. Braga MJ., Oliveira I., Egipto P., et al. High-voltage electrical burns due to copper theft – case series. Ann Burns Fire Disasters. 2016, 29(1): 41–42.
10. Liu HY., Zhang MQ., Wang RX., et al. Experiences in the treatment of electrical burns covering deep wounds with various tissue flaps. Acta Chir Plast. 1989, 31(4): 209–225.
11. Zhu ZX., Zhang YT., Liu XY., et al. Urgent repair of electrical injuries: analysis of 40 cases. Acta Chir Plast. 1990, 32(3): 142–151.
12. Buja Z., Arifi H., Hoxha E. Electrical burn injuries. An eight-year review. Ann Burns Fire Disasters. 2010, 23(1): 4–7.
13. Zhu ZX., Wang Y., Liu XY., et al. Repair of experimental high voltage electrical injuries. Acta Chir Plast. 1990, 32(2): 99–106.
14. Kapounková Z., Tvrdek M., Váchal J. Reconstruction of a devastating electric injury: case-report. Acta Chir Plast. 1993, 35(3–4): 118–124.
15. Al-Benna S., Alzoubaidi D., Al-Ajam Y. Evidence-based burn care – an assessment of the methodological quality of research published in burn care journals from 1982 to 2008. Burns. 2010, 36(8): 1190–1195.
16. Al-Benna S., Al-Ajam Y., Way B., et al. Descriptive and inferential statistical methods used in burns research. Burns. 2010, 36(3): 343–346.
17. Al-Benna S., Al-Ajam Y., Way B., et al. Deployment of patient database software for research in burns care. Burns. 2009, 35: S44.
18. Al-Ajam Y., Al-Benna S. Burns associations and societies websites – do they provide enough information for patients and doctors? Burns. 2009, 35: S42.
19. Al-Benna S., Patani N., Al-Ajam Y. Burns is not in the core curricula of medical schools in the United Kingdom. Burns. 2008, 34(6): 902.
20. Al-Benna S., Al-Ajam Y. The preferences of patients with respect to their burns care. Burns. 2009, 35: S30.
21. Al-Benna S., Patani N., Al-Ajam Y. Burns is not in the core curricula of medical schools in the United Kingdom. Burns. 2008, 34(6): 902.
22. Al-Benna S., Al-Ajam Y., Alzoubaidi D. Burns surgery handover study: trainees’ assessment of current practice in the British Isles. Burns. 2009, 35(4): 509–512.
23. Al-Benna S. Construction and use of wound care guidelines: an overview. Ostomy Wound Manage. 2012, 58(8): 37–47.
24. Al-Benna S. A discourse on the contributions of evidence-based medicine to wound care. Ostomy Wound Manage. 2010, 56(6): 48–54.
25. Tvrdek M., Nejedlý A., Kletenský J., et al. Use of free flaps in burn trauma. Acta Chir Plast. 1994, 36(1): 19–23.
26. Lipový B., Kaloudová Y., Ríhová H., et al. High voltage electrical injury: an 11-year single center epidemiological study. Ann Burns Fire Disasters. 2014, 27(2): 82–86.
27. Mager R., Ríhová H. Successful treatment of a critically burned patient (case report). Acta Chir Plast. 2003, 45(3): 77–80.
28. Kaloudová Y., Rihová H., Brychta P., et al. Mutilating electrotrauma – case report. Acta Chir Plast. 2008, 50(1): 11–15.
29. Al-Benna S. Burn care facilities are lacking at major trauma centres in England. Burns. 2013, 39(3): 533.
30. Al-Benna S. Adequate specialised burn care services are essential at major trauma centres. Burns. 2013, 39(7): 1495–1497.
31. Al-Benna S., O’Boyle C. Burn care experts and burn expertise. Burns. 2014, 40(2): 200–203.
32. Al-Benna S. The paradigm of burn expertise: scientia est lux lucis. Burns. 2014, 40(6): 1235–1239.
33. Al-Benna S., Tariq G. Wound care education in the developing world. Wounds Middle East. 2017, 4 : 6–7.
34. Mihailidis TH., Al-Benna S. Examining trends in the evidence base for the treatment of burns and a quality assessment of randomised controlled trials over an 11-year period. Burns. 2022, 48(4): 753–761.
35. Al-Benna S. Rural plastic surgery. Ann Plast Surg. 2021, 87(2): 230.
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2023 Issue 2
- Possibilities of Using Metamizole in the Treatment of Acute Primary Headaches
- Metamizole vs. Tramadol in Postoperative Analgesia
- Spasmolytic Effect of Metamizole
- Metamizole at a Glance and in Practice – Effective Non-Opioid Analgesic for All Ages
- Safety and Tolerance of Metamizole in Postoperative Analgesia in Children
Most read in this issue
- Electrical burns in adults
- Objective and subjective assessment of Dupuytren's contracture
- The effect of smoking and elderly age on digital replantation – a multivariate analysis
- Median nerve entrapments in the forearm – a case report of rare anterior interosseous nerve syndrome