
Objective and subjective assessment of Dupuytren's contracture
Authors:
J. Menoušek 1,2; Z. Dvořák T. Šácha 1,2 2
Authors‘ workplace:
Department of Plastic and Aesthetic Surgery, St. Anne's University Hospital in Brno, Czech Republic
1; Faculty of Medicine, Masaryk University, Brno, Czech Republic
2
Published in:
ACTA CHIRURGIAE PLASTICAE, 65, 2, 2023, pp. 74-78
doi:
https://doi.org/10.48095/ccachp202374
Introduction
Dupuytren's contracture (DC) is a relatively common disease. It is a benign, slowly progressive fibroproliferative disease of the palmar aponeurosis or other sites (plantar aponeurosis – morbus Lederhose, penile aponeurosis – Peyron's disease) [1]. However, it carries many uncertainties, its aetiology is not clearly defined and there are different opinions on treatment. It is characterised by the formation of knots and bands in the palmar and digital fascia, which shorten and lead to contracture of the fingers, thereby limiting hand function [2]. The disease is named after the French surgeon Guillaume Dupuytren, who described and published facts on the disease in detail in 1831 [3].
In 1959, Luck divided the progression of the disease into three stages [4]. The first stage – proliferative, fibroblastic proliferation and nodule formation. Second stage – involutional, fibroblasts are not regulated and transform into myofibroblasts. Third stage – residual stage, type III collagen begins to deposit and this connective tissue begins to organise into bands that subsequently contract. There is a relative excess of type III collagen over type I collagen.
Due to the different stages of disease development in patients, there is a need to classify the different clinical pictures of the disease development. Over the years, different classification schemes with variable disease specificity have been developed. For the surgeon, it is crucial to objectify the condition before starting the treatment and to evaluate the results after a certain precise period of time in order to select the right treatment method. Treatment recommendations vary around the world and relate to patient preference and surgeon expertise. Guidelines for the appropriate treatment of each stage of the disease are still lacking. As each author prefers different classification schemes, it is challenging to compare individual study results with each other on a global level. For this reason, any work evaluating disease classification is important.
Disease recurrence and Dupuytren's diathesis are complications that doctors encounter and it is good to be prepared for them. The first to introduce the concept of Dupuytren's Diathesis was Hueston in 1963. It is a condition where a patient with Dupuytren's contracture tends to have a more aggressive form and a greater risk of disease recurrence after surgery. The following four factors are considered to be risk factors: bilateral disease; family history of Dupuytren's disease; ectopic lesions and age at onset [5]. Hindocha found that patients with five risk factors (male sex, bilateral lesions, ectopic form, age < 50 years and positive family history) had a 71% chance of disease recurrence compared to patients without a risk factor in whom the likelihood is 21% only [6].
The aim of the work was to get an overview of the different classification schemes that are commonly used and, if possible, to select the most suitable one for both the patient and the physician.
The search was performed using the web PubMed.gov [7] where the MeSH Database was searched for the keywords "contracture, dupuytren", and "classification", which were selected from the Subheadings. A total of 40 articles from the years 1967–2022 were found. This search was narrowed down by the keywords: "(scoring) OR (assessment) OR (staging)", which brought a result of 28 articles from 1978–2022. For all of these articles, the abstract was read by the authors and articles that contained some classification schemes were retrieved, as well as source articles that contained information on the issue of classification schemes for Dupuytren's contracture. All these articles were usable for compiling this review article.
Assessment of the issue
From the relevant articles, five classifications and four questionnaires were evaluated. All the classifications listed below were produced since the year 1936 up to the present. Patient questionnaires have been developed over time in the last 30 years.
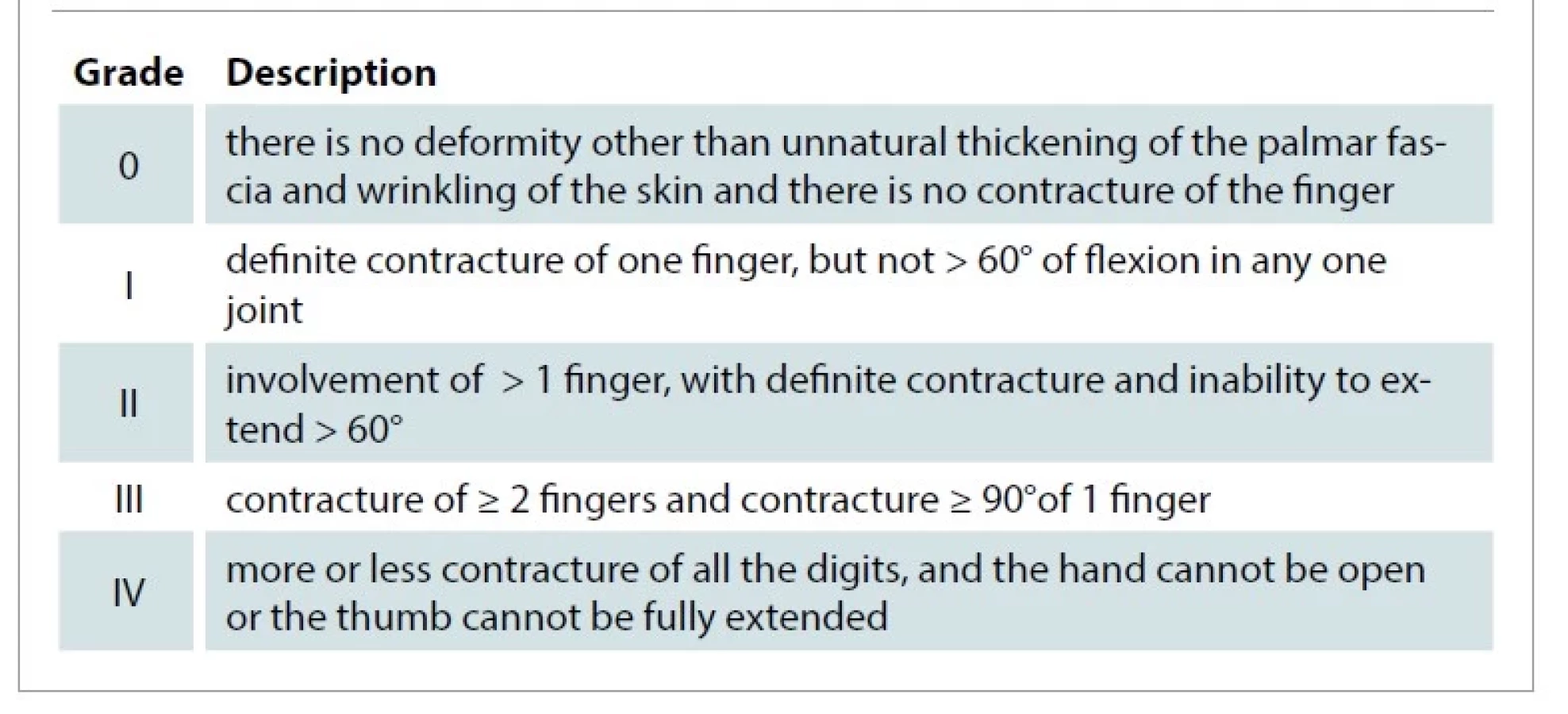
The Meyerding classification was published in 1936 and is the oldest scheme for Dupuytren's contracture that has been traced [8]. It consists of five grades: zero, one, two, three and four (Tab. 1).
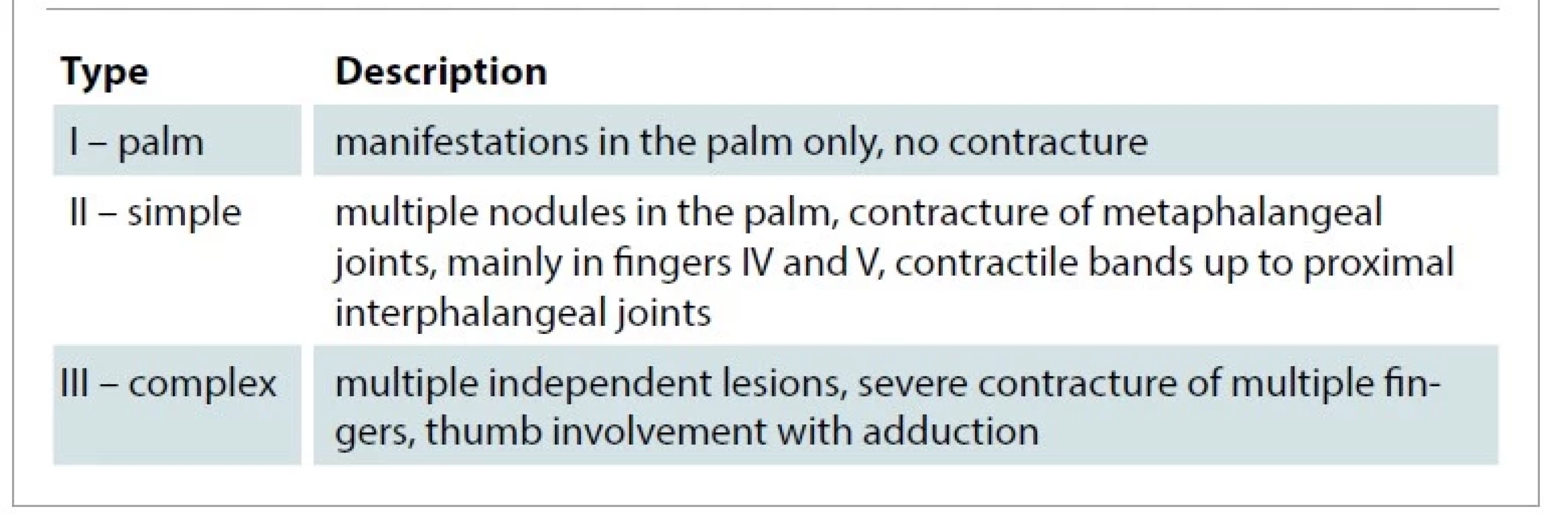
The Karfík classification is the most well-known classification in Czechia [9]. This classification was published in Dr. Karfík's dissertation in 1948 and, despite its popularity, it is not very accurate and does not allow to assess the postoperative outcome. The classification consists of three types of hand involvement: palm, simple, and complex types (Tab. 2).
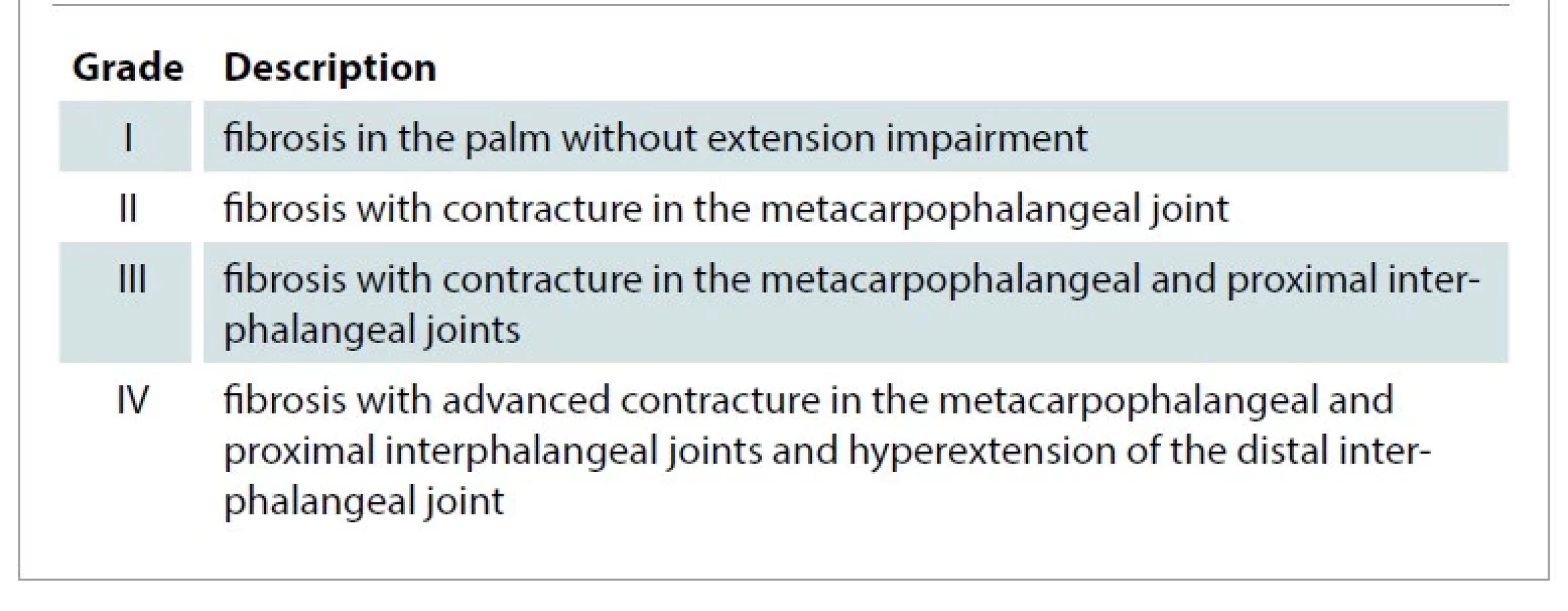
The Iselin classification is another frequently used classification [10]. The first version was published together with Dieckmann in 1951. It was intended to serve as a basis for surgical indications and selection of a surgical method. As this first version did not meet these conditions, the author began to modify it in 1955, and from 1958, this classification was taught in courses in Nanterre. According to the author, it is easy to understand and remember because each of its elements corresponds to an easily recognizable clinical aspect and a specific therapeutic approach. It was not published until 1967 in the Traité de Chirurgie de la Main. It was widely used in French-speaking countries. The classification is divided into four grades: first, second, third and fourth (Tab. 3).
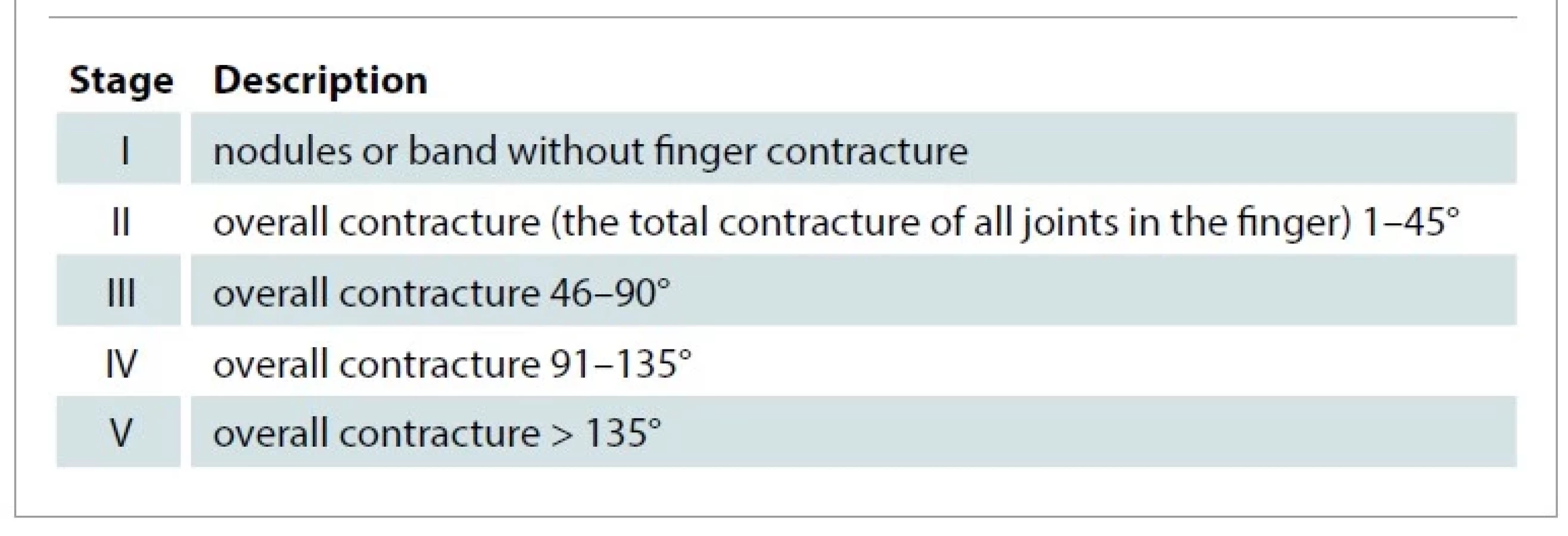
Mikkelson's classification is based on Tubiana's original work from 1968, when the scoring of individual disease stages was abandoned [11]. This simplified classification was published in 1976 as a part of an epidemiological study of the incidence of Dupuytren's contracture in a small town in Norway. The classification is divided into 5 stages: first, second, third, fourth, and fifth (Tab. 4).
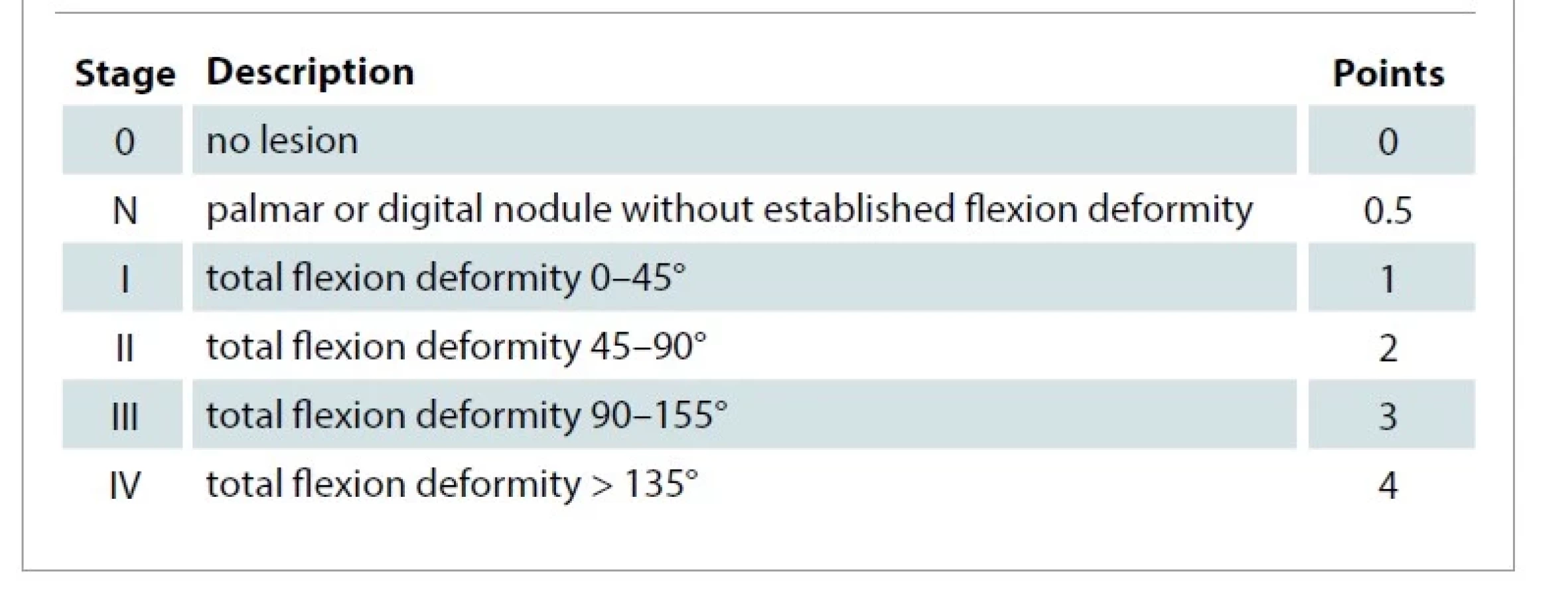
The Tubiana classification is the most commonly used and appears to be the most accurate. Published in 1968, it originally consisted of a classification for the fingers only and has gradually evolved to its present form [12]. The different stages are graded by 45° of flexion contracture and are divided into six grades: null, nodular, first, second, third and fourth. For each finger, we are able to detect the disability from 0° (physiological finding) to 200° (finger to palm contracture). Later, the individual degrees of contracture were scored from 0.5 to 4 points [13] (Tab. 5).
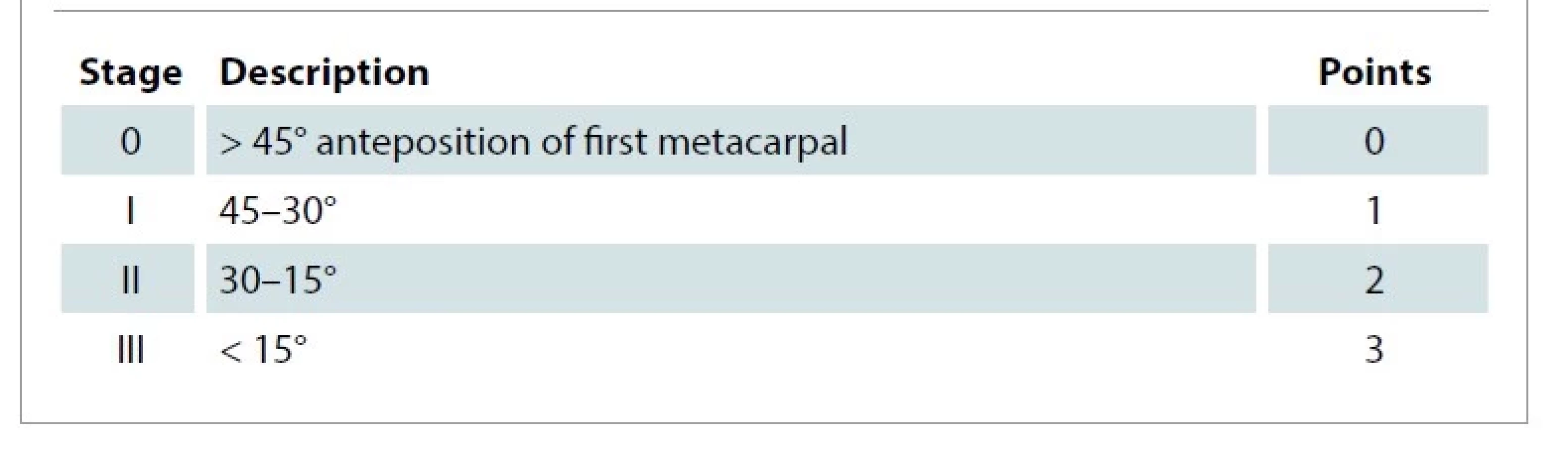
Furthermore, a classification for the 1st interdigital space was defined with a four-level scheme and scoring. We evaluate the angle between the 1st and 2nd metacarpal when the physiological angle is 45° or more. Each grading level represents a loss of full extension of 15°. On the thumb, we can measure flexion contracture in the metaphalangeal and the interphalangeal joint ranging from 0–160°, and the contracture of the 1st metacarpal joint ranging from 0–45° (Tab. 6).
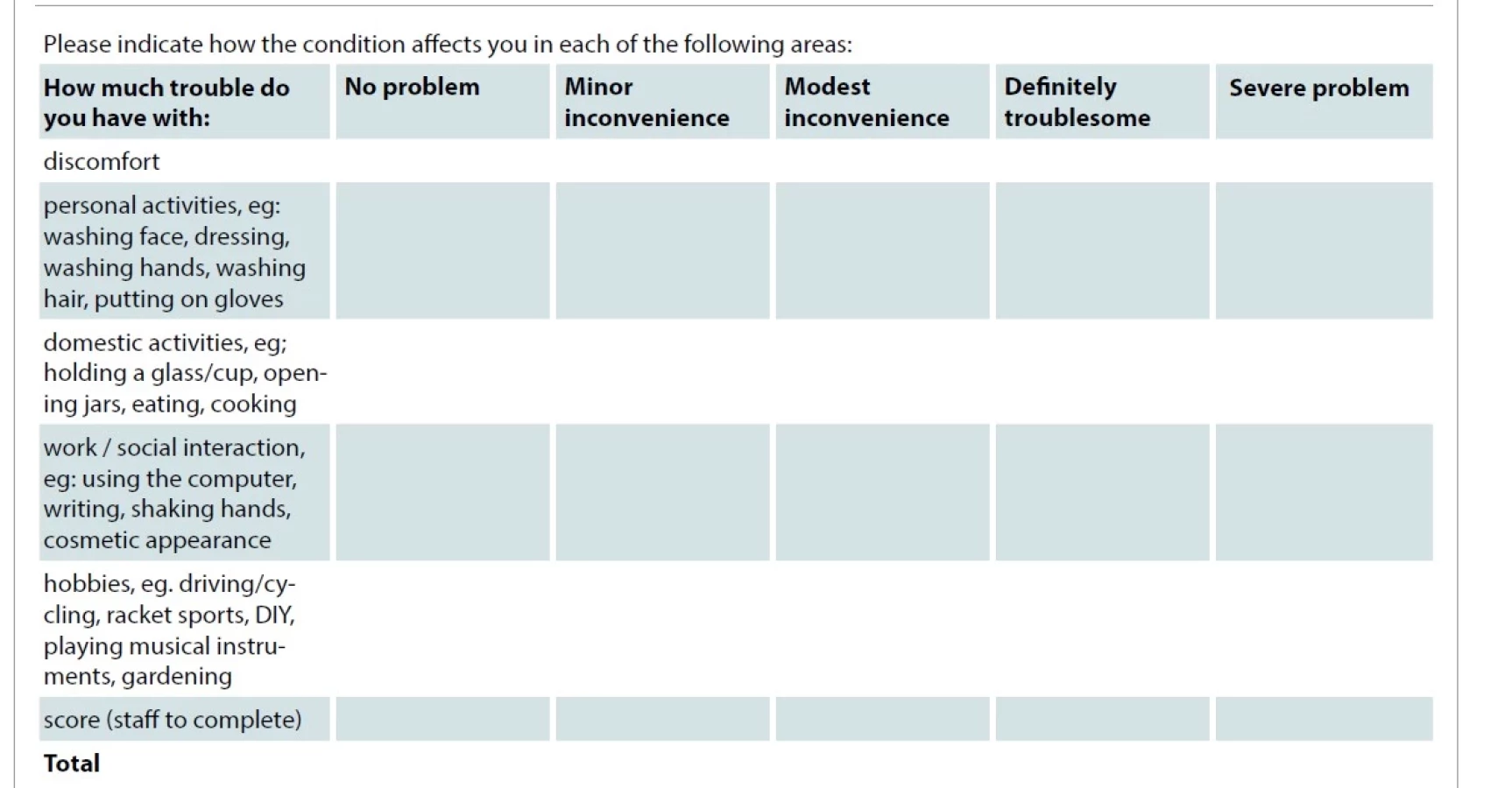
In addition to the physical evaluation of Dupuytren's contracture, there is also a subjective evaluation in the form of a questionnaire for patients. The most commonly used questionnaire for the evaluation of the upper extremity musculoskeletal disorders is (Tab. 7) the QuickDASH questionnaire [14]. It is a shortened questionnaire with 11 questions, based on the Disabilities of Arm, Shoulder and Hand (DASH) questionnaire with 30 questions [15]. The questionnaires are valid, reliable and selective. They can be used for clinical trials and for research. The questionnaires have been translated into most of the world's languages and to date have been translated into 55 languages and dialects. The greatest disadvantage is their low specification for Dupuytren's contracture. The questionnaire is free to download for academic and research users [16]. The Michigan hand outcomes questionnaire (MHQ) is another questionnaire being used [17]. This questionnaire consists of 37 questions (Tab. 8) that are divided into 6 groups (overall hand function, activities of daily living, pain, work performance, aesthetics, and patient satisfaction with the outcome). The questionnaire is free after registration for academic and research users [18]. Higher specification appears to be found in the Southampton Dupuytren's Scoring Scheme (SDSS) questionnaire (Tab. 7) [19] the aim of which was to construct a simple scheme to quantify disability and ensure sensitivity to changes in Dupuytren's contracture. The questionnaire consists of five questions, which are divided as follows: discomfort, personal activities, home activities, work and social interactions, and hobbies. These questions can be answered on a five-point scale ranging from no difficulty to great difficulty.
Discussion
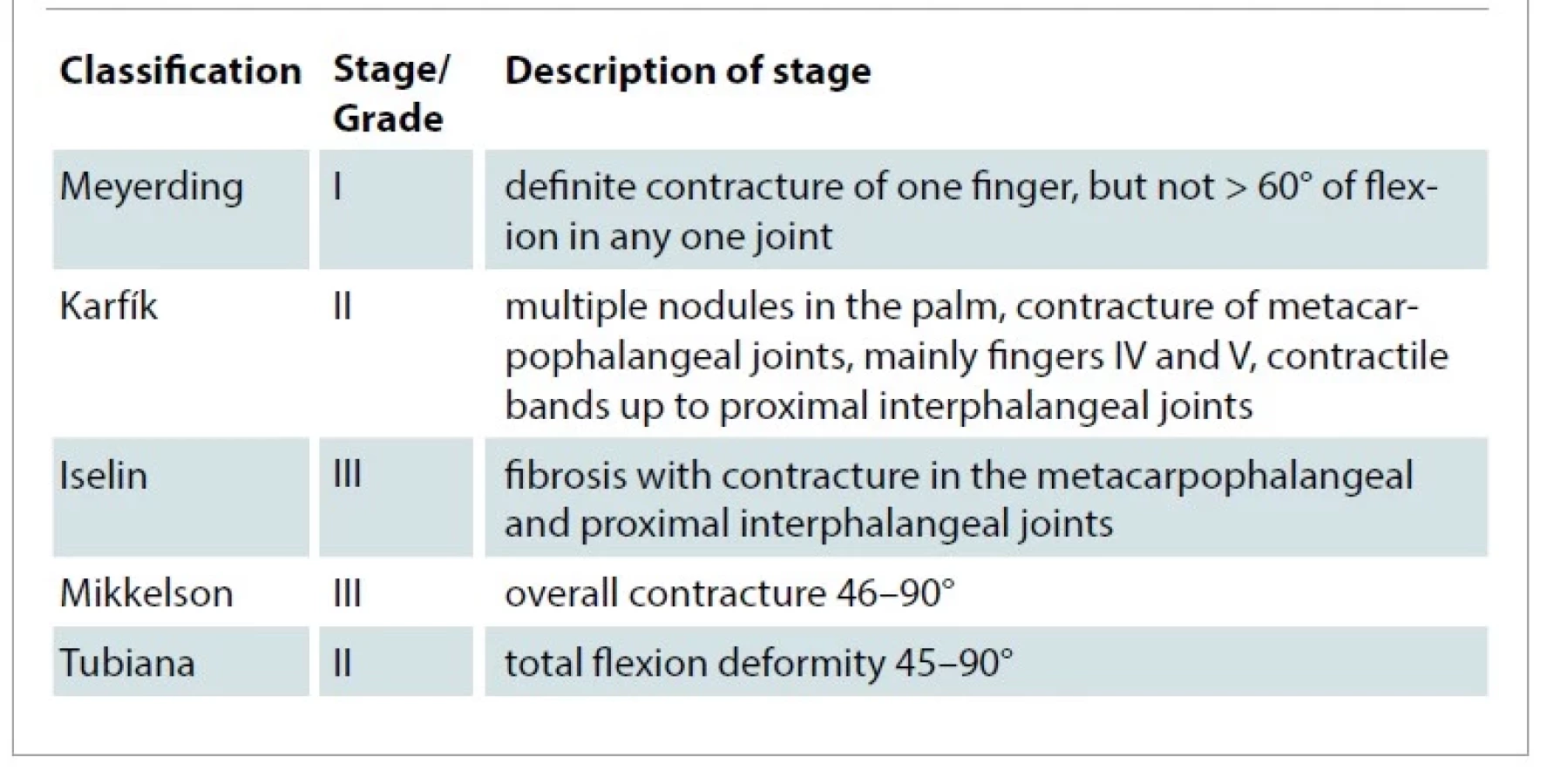
In an effort to incorporate new technologies that could potentially simplify, among other things, searching of articles, we have tried to use artificial intelligence, specifically, the ChatGPT chatbot from OpenAI launched in November 2022 [20]. This groundbreaking AI tool has become the fastest growing application with > 100 million monthly users worldwide [21]. It has been able to provide us with a large database of studies containing various forms of Dupuytren's contracture classifications. Unfortunately, subsequent efforts to track down these articles revealed that it had probably artificially created some of them. It will certainly be a very helpful tool for future research, but cannot be fully relied upon at present. For this reason, the articles were searched using the PubMed.gov database. Of the five classification schemes listed above, the Karfík classification, which is simple, clear and easy to remember, was most commonly used in Czechoslovakia. Unfortunately, it is not useful for the prognosis of the disease and for evaluation after surgery. Worldwide, the Tubiana classification is most commonly used. Both for its completeness, accuracy and for its scoring, we were able to assess the condition before and after surgery. Currently, in the Czech Republic, the older and younger generations of physicians use the Karfík and the Tubiana classifications, respectively. The impossibility of comparing the results of the treatment of patients between individual centres due to inconsistent use of classifications belongs to its major disadvantages. The commonly used MHQ, DASH and QuicDASH questionnaires for the evaluation of musculoskeletal disorders of the upper limb are also used in the evaluation of Duputren's contracture. Unfortunately, these questionnaires are not the most appropriate for this type of disorder due to their low specificity. In response to this finding, the SDSS questionnaire was developed. Compared to the QuickDASH, it is more specific for the disease of Dupuytren's contracture and appears to be a non-random questionnaire for patients with this condition. The author's experience with the classification schemes listed above is as follows: the Karfík classification is very general, but sufficient for basic assessment of the condition. In contrast, the Tubiana classification is more complex and considerably more precise and essential for scientific work. Independence is another important part in the measurement; the author recommends that the measurements should be performed by a trained physiotherapist. The comparison of all classification schemes in one patient is summarised in Fig. 1 and Tab. 8.
Range of motion: metacarpophalangeal joint 0–0–90°, proximal
interphalangeal joint 0–50–95°, distal interphalangeal joint 0–0–65°

Conclusion
Patient classification at entry to treatment and outcome measurement at follow-up should be an integral part of any treatment plan. Among the questionnaires for patients with Dupuytren's contracture, the SDSS seems to be the best for comparing the success of the treatment.
Disclosure: This study was supported by an internal specific grant of St. Anne's University Hospital in Brno: FNDN_IP21IPV16AXA_PN, 01699800. Evaluation of innovative procedures in plastic and reconstructive surgery III (MUNI/A/1360/2022), Evaluation of innovative procedures in plastic and reconstructive surgery II (MUNI/A/1457/2021). All procedures performer in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Roles of authors: Jan Menoušek and Tom Šácha conducted the literature search, designed the flowchart and analysed the collected data.
Jan Menoušek wrote the manuscript with the input from all authors.
Zdeněk Dvořák conceived the study and revised it critically for important intellectual content.
All the authors approved the version to be published.
Jan Menoušek, MD
Department of Plastic and Aesthetic Surgery
St. Anne's University Hospital in Brno
Pekařská 664/53
602 00 Brno
Czech Republic
e-mail: jan.menousek@fnusa.cz
Submitted: 4. 4. 2023
Accepted: 26.7. 2023
Sources
1. Krejča M., et al. Ektopické léze. In: Dupuytrenova nemoc. 2. doplněné a přepracované vydání. Praha: Grada Publishing 2017 : 43–46.
2. Haase S., Chung KC. Dupuytren disease, an issue of hand clinics. Elsevier Health Sciences 2018.
3. Elliot D. The early history of contracture of the palmar fascia. Part 2: the revolution in Paris: Guil-laume Dupuytren: Dupuytren’s disease. J Hand Surg Br. 1988, 13(4): 371–378.
4. Luck JV. Dupuytren’s contracture; a new concept of the pathogenesis correlated with surgical management. J Bone Joint Surg Am. 1959, 41-A(4): 635–664.
5. Hueston JT. Recurrent Dupuytren’s contracture. Plast Reconstr Surg. 1963, 31 : 66–69.
6. Hindocha S., Stanley JK., Watson S., et al. Dupuytren’s diathesis revisited: evaluation of prognostic indicators for risk of disease recurrence. J Hand Surg Am. 2006, 31(10): 1626–1634.
7. https://pubmed.ncbi.nlm.nih.gov/.
8. Meyerding HW. Dupuytren’s contracture. Arch Surg. 1936, 32(2): 320–333.
9. Karfík V. Dupuytrenova kontraktura: studie a operační návod. Praha: Spol. č. lékařů 1949.
10. Iselin M., Iselin F. Maladie de Dupuytren. In: Traité de chirurgie de la main. Paris: Éditions Médicales Flammarion 1967 : 667–713.
11. Mikkelsen OA. Dupuytren’s disease – a study of the pattern of distribution and stage of contracture in the hand. Hand. 1976, 8(3): 265–271.
12. Tubiana R., Michon J., Thomine JM. Scheme for the assessment of deformities in Dupuytren’s disease. Surg Clin North Am. 1968, 48(5): 979–984.
13. Tubiana R, Thomine JM, Mackin E. Examination of the Hand and Wrist. CRC Press; 1998. 412 p.
14. Beaton DE., Wright JG., Katz JN., et al. Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005, 87(5): 1038–1046.
15. Hudak PL., Amadio PC., Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996, 29(6): 602–608.
16. DASH. [online]. Available from: https://dash.iwh.on.ca/access/quickdash/122983.
17. Chung KC., Pillsbury MS., Walters MR., et al. Reliability and validity testing of the Michigan Hand Outcomes Questionnaire. J Hand Surg Am. 1998, 23(4): 575–587.
18. Michigan Hand Outcomes Questionnaire. [online]. Available from: https://umich.flintbox.com/technologies/8089f106-43b8-469a-9228-a99e14d2e5f3.
19. Mohan A., Vadher J., Ismail H., et al. The Southampton Dupuytren’s Scoring Scheme. J Plast Surg Hand Surg. 2014, 48(1): 28–33.
20. Introducing ChatGPT. [online]. Available from: https://openai.com/blog/chatgpt.
21. What Is ChatGPT? A review of the AI in its own words – Forbes advisor. [online]. Available from: https://www.forbes.com/advisor/business/software/what-is-chatgpt/.
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2023 Issue 2
- Possibilities of Using Metamizole in the Treatment of Acute Primary Headaches
- Metamizole at a Glance and in Practice – Effective Non-Opioid Analgesic for All Ages
- Metamizole vs. Tramadol in Postoperative Analgesia
- Spasmolytic Effect of Metamizole
- Safety and Tolerance of Metamizole in Postoperative Analgesia in Children
Most read in this issue
- Electrical burns in adults
- Objective and subjective assessment of Dupuytren's contracture
- The effect of smoking and elderly age on digital replantation – a multivariate analysis
- Median nerve entrapments in the forearm – a case report of rare anterior interosseous nerve syndrome