
Effect of vacuum-compression therapy for carpal tunnel syndrome as a part of physiotherapy – pilot study
Využití vakuově-kompresní terapie v léčbě syndromu karpálního tunelu jako součást fyzioterapie – pilotní studie
Cíl: Cílem této pilotní studie bylo vyhodnotit efekt kombinace kinezioterapie a vakuově-kompresní terapie u pacientů se syndromem karpálního tunelu (carpal tunnel syndrome; CTS). Sekundárním cílem bylo sledovat korelaci mezi subjektivními příznaky a výsledky objektivního měření.
Metodika: Deset pacientů (šest žen; věkový průměr 55,0 ± 12,7 roku) s osmnácti hodnocenými horními končetinami, indikovaných k chirurgické léčbě CTS, absolvovalo šest individuálních kinezioterapií a deset aplikací vakuově-kompresní terapie. Efekt intervence byl hodnocen pomocí EMG a vizuální analogové škály bolesti.
Výsledky: Výsledky EMG neprokázaly po terapii statisticky významné rozdíly v měření distální motorické latence, velikosti senzitivní amplitudy a senzitivní rychlosti vedení vzruchu. Velikosti hodnot na vizuální analogové škále bolesti se však signifikantně snížila (p = 0,001). V měřených parametrech CTS jsme nalezli velké inter-individuální rozdíly. Devět pacientů nepodstoupilo chirurgickou léčbu ještě rok po ukončení intervence.
Závěr: Po terapii sestávající z kinezioterapie a vakuově-kompresní terapie došlo ke snížení výskytu typických příznaků CTS.
Autoři deklarují, že v souvislosti s předmětem studie nemají žádné komerční zájmy.
Redakční rada potvrzuje, že rukopis práce splnil ICMJE kritéria pro publikace zasílané do biomedicínských časopisů.
Klíčová slova:
syndrom karpálního tunelu – kinezioterapie – vakuově-kompresní terapie
Authors:
R. Poděbradská 1,2; M. Janura 3; J. Průcha 4; M. Nevrlý 5; M. Elfmark 3; E. Minks 6
![]()
Authors‘ workplace:
Rehabilitace REHEX – EDU, v. o. s., Lipová-lázně
1; Department of Health Promotion, Faculty of Sports Studies, Masaryk University, Brno, Czech Republic
2; Department of Natural Sciences in Kinanthropology, Faculty of Physical Culture, Palacký University, Olomouc, Czech Republic
3; Department of Health Care Disciplines and Population Protection, Faculty of Biomedical Engineering, Czech Technical University in Prague, Czech Republic
4; Department of Neurology, University Hospital in Olomouc, Czech Republic
5; First Department of Neurology, Faculty of Medicine, Masaryk Univerzity and St. Anne´s Faculty Hospital, Brno, Czech Republic
6
Published in:
Cesk Slov Neurol N 2019; 82(3): 345-348
Category:
Short Communication
doi:
https://doi.org/10.14735/amcsnn2019345
Overview
Aim: The aim of this pilot study was to assess the effect of combined kinesiotherapy and vacuum-compression therapy (VCT) in patients with carpal tunnel syndrome (CTS). A secondary aim was to evaluate the correlation between subjective symptoms and the results of objective measurements.
Methods: Ten patients (six women; average age 55.0 ± 12.7 years) with a total of 18 hands, indicated for the surgical treatment of CTS underwent six individual kinesiotherapy sessions and ten applications of VCT. The effect of the intervention was evaluated by EMG and a visual analogue scale (VAS) of pain.
Results: After the therapy, EMG did not show a statistically significant difference in distal motor latency, sensory nerve action potential and sensory conduction velocity of the median nerve. However, the VAS decreased significantly (P = 0.001). We found immense inter-individual differences in measurable parameters of the manifestations of CTS. Additionally, none of the patients opted for surgical treatment even one year after finishing the therapy.
Conclusion: After therapy consisting of kinesiotherapy and VCT, the typical symptoms of CTS decreased.
真空压缩治疗腕管综合征的疗效作为物理治疗的一部分-初步研究
目的:
本研究的目的是评估运动疗法和真空压缩疗法(VCT)联合治疗腕管综合征(CTS)的效果。第二个目的是评估主观症状与客观测量结果之间的相关性。
方法:
10名患者(6名女性;平均年龄(55.0±12.7岁),共18只手,手术治疗CTS需要6次单独运动疗法和10次VCT应用。采用肌电图(EMG)和疼痛视觉模拟量表(VAS)评价干预效果。
结果:
治疗后正中神经远端运动潜伏期、感觉神经动作电位、感觉传导速度肌电图无统计学差异。然而,VAS显著下降(P = 0.001)。我们发现CTS表现的可测量参数存在巨大的个体间差异。此外,没有患者选择手术治疗,甚至一年后完成治疗。
结论:
经运动疗法和VCT治疗后,CTS的典型症状有所减轻。
关键词:
腕管综合症-运动疗法-真空压缩疗法
Keywords:
carpal tunnel syndrome – kinesiotherapy – vacuum-compression therapy
Introduction
Carpal tunnel syndrome (CTS) is a set of symptoms caused by compression of the median nerve as it travels through the wrist in a space-limited osteofibrous canal (carpal tunnel) [1]. CTS is the most common entrapment syndrome in the general population [2–4]. The prevalence has been estimated at 6 to 12% [5] and the incidence is stated to be from 180 to 346 diagnosed cases per 100,000 people. It is one of the most frequent occupational diseases [6].
The aetiology of CTS is multifactorial; structural as well as functional factors operate in its occurrence, combining in different stages [7]. The direct cause of the occurrence of the typical symptoms of CTS is a pathological increase of intracarpal pressure. The compression of the well-developed microvascular system of blood vessels results in dysfunction of the affected nerve. If the disorder of the epineural blood flow lasts long enough, an oedema occurs in the epineurium and endoneurium, with a subsequent axonal transport blockade. Gradually, structural changes of the nerve also occur, especially segmental demyelination and remyelination of the compressed fibre [3,8].
To confirm the CTS, electrodiagnostic (electrophysiological) testing together with clinical evaluation is used most commonly. An EMG represents an available sensitive standardized method for examining median nerve dysfunction.
In an EMG for CTS, the values of distal motor latency, sensory nerve action potential and sensory conduction velocity are considered to be the most important indicators of the function of the median nerve [9–11]. Moderate CTS is diagnosed in cases of velocity of conduction via the sensitive fibres of the median nerve from the wrist to the 2nd or the 3rd finger as measured with an EMG reduced at least to 38 m/ s, or the response not being present. In addition, it is necessary to have a normal finding of distal motor latency and the conduction via sensitive fibres to the 5th finger by the ulnar nerve. Another necessary finding in this type of affection is either distal motor latency of the median nerve prolonged to 5.3 ms and more or the response not being present, and/ or the finding of permanent abnormal spontaneous activity in a needle EMG in the musculus abductor pollicis brevis, in at least two
locations [9].
There are several therapeutic options for patients with CTS depending on various factors, including the stage of the disease, the severity of the symptoms and patients’ preferences. Non-surgical intervention is recommended as the first-line treatment in cases of mild to moderate CTS. Conservative therapy includes medical and physical therapy [8,12]. Surgery is reserved for patients with severe CTS and those who have experienced a failure of conservative treatment. [12,13]. Surgical treatment consists of releasing the carpal tunnel content by transection of the transverse carpal ligament [4].
Vacuum-compression therapy (VCT) represents one of the methods used for physical therapy. The procedure, with cycles of vacuum and subsequent compression leads to increased capillary filling [14]. Therefore, the effects of VCT might target the primary cause of the occurrence of several types of CTS. However, no study has been conducted thus far which has documented the effect of this therapy on the improvement of CTS. The aim of this pilot study was therefore to assess the effect of a combination of kinesiotherapy and VCT in the treatment of CTS. The finding that the combination of kinesiotherapy and VCT has a positive effect might help to include this method in the CTS treatment algorithm.
Methods
Participants
Ten patients (six women; age 55.0 ± 12.7 years) with a diagnosis of idiopathic CTS in 18 hands, who had undergone conservative treatment, were included in the study. There were eight patients with bilateral symptoms and two patients with unilateral symp-
toms. All the patients presented with symptoms of median nerve compression. The symptoms included volar wrist pain, numbness, dysaesthaesia and paraesthaesia in the median nerve distribution. When the neurologist according to the EMG confirmed the diagnosis of moderate CTS and ruled out another neurological disease, all the patients were indicated for surgical treatment.
This study was conducted according to the principles for human experimentation of the Declaration of Helsinki. All the subjects provided written informed consent.
Procedure
The EMG was performed by an experienced neurophysiologist at a clinical site using a Keypoint machine (Medtronic Inc., Minneapolis, MN, USA) according to the methodology recommended by the Czech Neurological Society [9,10]. The median nerve was stimulated by a surface electrode in the area of the wrist and the motor response was read from the abductor pollicis brevis muscle. The technique of antidromic conduction with stimulation of the median nerve in the area of the wrist was used to examine sensitive conduction and the response was read by ring surface electrodes from the index finger. The measured EMG parameters were distal motor latency, sensory nerve action potential and sensory conduction velocity of the median nerve. This examination was carried out no later than one month prior to starting the therapy and from one to three months after the therapy.
The therapy included 6 sessions of individual kinesiotherapy lasting 30 min each and 10 sessions of VCT. Individual kinesiotherapy was based on Dynamic Neuromuscular Stabilization, which is a manual and rehabilitative approach to optimize the movement system based upon the scientific principles of developmental kinesiology [7,15]. The machine used for VCT – Vasotrain-447 (Enraf-Nonius, Rotterdam, The Netherlands) can produce both positive and negative pressure, which have been used intermittently in vascular reeducations [14]. The involved upper limb was placed into the Vasotrain-447, the proximal part of the cylinder was fixed around the midpart of the upper arm with a rubber balloon and the machine was set for vascular disease. Treatment was started with 0.10 bar of negative pressure for 60 s, followed by 0.01 bar of overpressure for 60 s. These parameters were then increased by 0.01 bar in each session. However, the pressure was not further increased when it was no longer within the patient’s tolerance and comfort or the colour of the skin on the forearm in the machine changed.
The overall length of the therapy did not exceed one month.
After one year had elapsed after the second EMG examination, a further course of treatment was inquired about by an outpatient neurological department.
The pain intensity was assessed by a Visual Analogue Scale (VAS) before starting the therapy and 1–3 months after the therapy as a part of EMG examination.
Statistical analysis
Statistical analyses were performed using the Statistica version 12.0 (StatSoft, Inc., Tulsa, OK, USA) software. The normality of the data distribution was assessed using the Lilliefors test. Because the data were not normally distributed, the Mann-Whitney U test was used to compare the outcomes at baseline and after the therapy. The value of the r score (rsc = Z/ sqrt[N], where N is the total number of observations) was used to evaluate the effect size; the effect size was considered large for values ≥ 0.5 and moderate for values ≥ 0.3 and < 0.5 [16]. A correlation analysis (Spearman correlation coefficient) was used to assess the relationship between the VAS and the distal motor latency, sensory nerve action potential and sensory conduction velocity of the median nerve. The significance level was set at 0.05 for all statistical tests.
Results
Effect of the intervention
The basic statistical characteristics of the monitored parameters are given in Tab. 1.
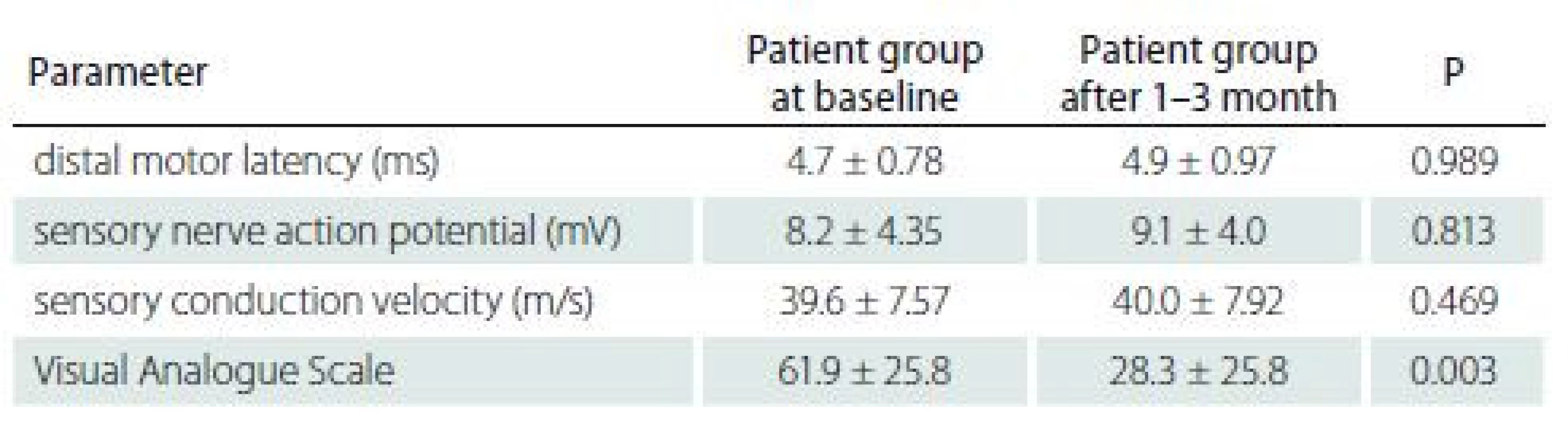
Table 1 shows that after the therapy there were no statistically significant changes in the EMG parameters. However, the subjective difficulties decreased significantly after 1–3 months when compared to the baseline (P = 0.003, rsc = 0.706).
Relationship between EMG parameters and VAS
In the follow-up measurement after 1–3 months, we found a significant relationship between the intensity of the subjective difficulties and the sensory conduction velocity (r = – 0.659, P = 0.004) and between the intensity of the subjective difficulties and the distal motor latency (r = 0.704, P = 0.002).
Discussion
Carpal tunnel syndrome is a multifactorial disease which includes functional and structural aetiology in different proportions. This proportion should be determined in order to determine the options for treatment, either conservative or surgical. The positive effect of conservative therapy of CTS has been demonstrated repeatedly [17–20], in improved function as well as nerve conduction [21].
The decrease of typical symptoms of CTS, which occurs after conservative therapy is, in many cases, only temporary [22]. Therefore, in our study we tried to add conservative therapy with another method – VCT, which could support the results of conservative therapy and lead to a longer-term effect. All the patients were indicated for the surgical treatment of CTS based on their symptoms and the results of the EMG.
The results of our study did not show any significant change in the EMG parameters, but there was a statistically significant improvement of the subjective CTS symptoms. The improvement of the subjective clinical symptoms may have been induced by the improved movement stereotype in the area of the upper limb, i.e. the influence of the functional aetiology of CTS, whereas the actual regeneration of the peripheral nerve, which would be measurable objectively, requires a longer time [23]. Functional disorders of the musculoskeletal system may also contribute to the clinical manifestation of CST [7].
A statistically significant relationship was found between changes in subjective symptoms and in distal motor latency. Such a finding is interesting, because in clinical practice, we meet patients with moderate CTS and minimal typical symptoms and conversely, also patients with mild CTS and very strong clinical problems. Therefore, we do not find it common that these two indicators must necessarily correlate.
The use of VCT for the treatment of CTS has not been described in available literature. Nevertheless, this treatment with a physical appliance using the energy of computer-controlled switching of the local hyperbaric and hypobaric environments is demonstrably effective in peripheral disorders of blood perfusion [14]. This is also confirmed by the results of a randomized study by Khadir et al [24] with the examination of peripheral vascular functions before and after the therapy. VCT may reduce the increased pressure in the carpal tunnel in CTS through its antioedematous effect, and during conservative therapy, it may support the regeneration of a nerve damaged by compression. However, it should not be indicated as monotherapy, as it does not aim at the cause of the occurrence of CTS. The study by Pitr et al [25] represents a comprehensive study including the results of biophysical experiments as well as a number of case studies. By marking the erythrocytes with technetium radionuclide and subsequently scanning the limb with a gamma camera, the authors demonstrated an improvement in the blood perfusion of the treated limb. This was also confirmed by experiments showing the improvement of microcirculation in the skin using skin remission spectrophotometry in vivo. Both mechanisms are important from the point of view of supplying oxygenated blood to the limb. A study quantifying the impact of VCT on the increased amount of oxygen being supplied to the treated limb was published by Ticháček et al [26]. This study used the results of earlier biomedical experiments and evaluated them afresh, using the findings from physiology and simulating methods of medical biophysics. The resulting findings confirm the significant impact of VCT on the support of peripheral perfusion, also suggesting a positive impact on the support of perfusion in the area of the vasa nervorum, therefore supporting the regeneration of the ischemized peripheral nerve.
Treatment of CTS by VCT and physiotherapy represents only one of the options of evidence-based conservative treatment, which also includes splinting and local injections of corticosteroids. VCT should be reserved for patients with mild to moderate CTS who are not indicated for surgery. In the pilot study, VCT therapy did not lead to the improvement of objective electro-physiological parameters in 1–3 months after the initiation of treatment.
Limitations of the study and therapy
When VCT is applied with the Vasostrain, the pressure in the rubber balloon does not change with the change of pressure in the cylinder. The patients perceive this pressure as very unpleasant. Optionally, it is possible to use the Extremiter (Madisson s.r.o., Prague, Czech Republic) appliance, which changes the pressure in the sleeve during the changes of the individual stages of overpressure and under pressure, and therefore the vascular connection with the proximal part of the upper limb outside the cylinder is not altered as much.
We are aware that the study lacked a control group of patients. Due to the high pain intensity, the majority of the patients from the control group (kinesiotherapy only) opted for surgical treatment before the end of the experiment and therefore a comparison with the experimental group was not possible.
A 2-week course of physiotherapy or, more precisely, six therapeutic sessions, was determined experimentally on the basis of the therapist’s empirical experience, with respect to the possibilities the site offered. However, the number of therapeutic sessions is highly individual and does not allow for fixed setting. It is possible that some patients may need a higher number of therapeutic sessions to achieve a positive effect on the functions of the deep stabilization system.
The limit may also be a combination of therapeutic procedures, specifically physiotherapy and VCT. Nevertheless, the effect of both methods is mutually potentiated and they should therefore be applied in combination.
Conclusion
The application of the combination of kinesiotherapy and VCT decreased the intensity of pain but did not change the EMG parameters in patients with moderate forms of CTS. This application had a positive influence on the course of further therapy, so that the patients were no longer indicated for surgical treatment at the time of the neurological examination from 1 to 3 months after therapy. In addition, none of the patients underwent surgical treatment for 1 year after the discontinuation of treatment.
Further research using a larger sample size is necessary to confirm the therapeutic effect of VCT for CTS treatment; until then, VCT should always be indicated with physiotherapy only as a complement to conservative treatment.
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
The Editorial Board declares that the manuscript met the ICMJE “uniform requirements” for biomedical papers.
Accepted for review: 18. 1. 2019
Accepted for print: 5. 4. 2019
PhDr. Radana Poděbradská, Ph.D.
Rehabilitace REHEX – EDU, v.o.s.
Horní Lipová 254
790 63 Lipová-lázně
Czech Republic
e-mail: rehex@rehex-edu.cz
Sources
1. Wahab KW, Sanya EO, Adebayo PB et al. Carpal tunnel syndrome and other entrapment neuropathies. Oman Med J 2017; 32(6): 449–454. doi: 10.5001/ omj.2017.87.
2. Smrčka M, Vybíhal V, Němec M. Syndrom karpálního tunelu. Neurol praxi 2007; 8(4): 243–246.
3. Kurča E. Syndróm karpálného tunela. Cesk Slov Neurol N 2009; 72/ 105(6): 499–510.
4. Vaverka M. Karpální tunel a neurochirurg – zkušenosti po 2 200 operacích. Cesk Slov Neurol N 2012; 75/ 108(1): 44–50.
5. Fernández-de-Las-Peñas C, Cleland J, Palacios-Ceña M et al. Effectiveness of manual therapy versus surgery in pain processing due to carpal tunnel syndrome: a randomized clinical trial. Eur J Pain 2017; 21(7): 1266–1276. doi: 10.1002/ ejp.1026.
6. Minsk E, Minksová A, Brhel P et al. Profesionální syndrom karpálního tunelu. Neurol praxi 2014; 15(5): 234–239.
7. Poděbradská R, Machová L. Syndrom karpálního tunelu v kontextu funkčních poruch pohybového systému. Cesk Slov Neurol N 2018; 81/ 114(2): 174–179. doi: 10.14735/ amcsnn2018174.
8. Poděbradský J, Poděbradská R. Fyzikální terapie – manuál a algoritmy. Praha: Grada Publishing 2009.
9. Kadaňka Z, Dufek J, Hromada J. Standard elektrofyziologického vyšetření syndromu karpálního tunelu pro potřeby hlášení choroby z povolání. [online]. Available from URL: https:/ / www.czech-neuro.cz/ archiv/ clanek/ 4-Sy-karpalniho-tunelu/ index.html.
10. Ridzoň P, Ehler E, Urban P et al. Normativní hodnoty parametrů vedení pro nervus ulnaris a nervus medianus měřené standardizovaným způsobem. Cesk Slov Neurol N 2014; 77/ 110(2): 210–215.
11. Dufek J. Profesionální syndrom karpálního tunelu. Neurol praxi 2006; 7(5): 254–256.
12. Kamel DM, Hamed NS, Abdel Raoof NA et al. Pulsed magnetic field versus ultrasound in the treatment of postnatal carpal tunnel syndrome: a randomized controlled trial in the women of an Egyptian population. J Adv Res 2017; 8(1): 45–53. doi: 10.1016/ j.jare.2016.11.001.
13. Hashempur MH, Naseri M, Ashraf A. Carpal tunnel syndrome in lactation: a challenging issue. Women Health Bull 2015; 2(4): e31414. doi: 10.17795/ whb-31414.
14. McCulloch JM Jr. Vacuum-compression therapy for the treatment of an ischemic ulcer. Phys Ther 1993; 73(3): 165–169. doi: 10.1093/ ptj/ 73.3.165.
15. Frank C, Kobesova A, Kolar P. Dynamic neuromuscular stabilization & sports rehabilitation. Int J Sports Phys Ther 2013; 8(1): 62–73.
16. Cohen J. Statistical power analysis for the behavioural sciences. New York: Academic Press 1988.
17. Tal-Akabi A, Rushton A. An investigation to compare the effectiveness of carpal bone mobilisation and neurodynamic mobilisation as methods of treatment for carpal tunnel syndrome. Man Ther 2000; 5(4): 214–222. doi: 10.1054/ math.2000.0355.
18. Wolny T, Saulicz E, Linek P et al. Effect of manual therapy and neurodynamic techniques vs ultrasound and laser on 2PD in patients with CTS: a randomized controlled trial. J Hand Ther 2016; 29(3): 235–245. doi: 10.1016/ j.jht.2016.03.006.
19. Rozmaryn LM, Dovelle S, Rothman ER et al. Nerve and tendon gliding exercises and the conservative management of carpal tunnel syndrome. J Hand Ther 1998; 11(3): 171–179. doi: 10.1016/ S0894-1130(98)80035-5.
20. Oskouei AE, Talebi GA, Shakouri SK et al. Effects of neuromobilization maneuver on clinical and electrophysiological measures of patients with carpal tunnel syndrome. J Phys Ther Sci 2014; 26(7): 1017–1022. doi: 10.1589/ jpts.26.1017.
21. Goyal M, Mehta S, Rana N et al. Motor nerve conduction velocity and function in carpal tunnel syndrome following neural mobilization: a randomized clinical trial. Int J Health Allied Sci 2016; 5(2): 104–110. doi: 10.4103/ 2278-344X.180434.
22. Piazzini DB, Aprile I, Ferrara PE et al. A systematic review of conservative treatment of carpal tunnel syndrome. Clin Rehabil 2007; 21(4): 299–314. doi: 10.1177/ 0269215507077294.
23. Gupta R, Rowshan K, Chao T et al. Chronic nerve compression induces local demyelination and remyelination in a rat model of carpal tunnel syndrome. Exp Neurol 2004; 187(2): 500–508. doi: 10.1016/ j.expneurol.2004.02.009.
24. Khadir SA, Chatterjee SP. Effect of vacuum compression therapy on lower limb vascular parameters in people with type 2 diabetes. Int J Ther Rehabil 2015; 22(9): 421–426. doi: 10.12968/ ijtr.2015.22.9.421.
25. Pitr K, Průcha J, Resl V et al. Vakuově-kompresní terapie: hemodynamická metoda fyzikální léčby – pět let výzkumů a zkušeností. Rehabil fyz Lék 2001; 8(1): 18–32.
26. Ticháček J, Štvrtinová V, Gúth A et al. Kvantifikace vlivu vakuově-kompresní terapie na přímé zvýšení dodávky kyslíku léčené končetině. Rehabil fyz Lék 2013; 20(2): 95–108
Labels
Paediatric neurology Neurosurgery NeurologyArticle was published in
Czech and Slovak Neurology and Neurosurgery

2019 Issue 3
- Advances in the Treatment of Myasthenia Gravis on the Horizon
- Memantine in Dementia Therapy – Current Findings and Possible Future Applications
- Memantine Eases Daily Life for Patients and Caregivers
Most read in this issue
- Coin in the Hand Test for detection of malingering memory impairment in comparison with mild cognitive impairment and mild dementia in Alzheimer‘s disease
- Neuromuscular diseases and pregnancy
- Optical coherence tomography measurements of the optic nerve head and retina in newly diagnosed idiopathic intracranial hypertension without loss of vision
- Effect of vacuum-compression therapy for carpal tunnel syndrome as a part of physiotherapy – pilot study